Article Text

Abstract
Background Atrio-ventricular (AV) block is a rare event in young-middle aged adults, often leading to pacemaker implantation without further investigation. We sought to assess the clinical utility of CMR in young-middle aged adults with high-grade AV block.
Methods We retrospectively analysed the CMR registry to collect data on consecutive high-grade AV block patients (18–60yrs) referred for CMR (September 2012–November 2015). High-grade AVB was defined as Mobitz II 2nd degree or complete AVB. All patients underwent a transthoracic echocardiogram (TTE) and a comprehensive CMR protocol (cine and late gadolinium enhancement, LGE). A change in diagnosis was defined as a new diagnosis compared to a multi-parametric pre-CMR diagnosis (based on clinical, ECG and TTE data).
Results We identified 34 patients (20 male, mean age 44 ± 12 years); 12 patients (34%) had II degree AVB and 22 (66%) complete AVB. Patients were referred to CMR for suspected ischaemic heart disease (IHD) in 4 patients (11%) and non ischaemic heart disease (NIHD) in 24 (71%); in 6 patients (18%) pre-CMR diagnosis was unclear. CMR showed IHD in 3 patients (9%) and NIHD in 11 patients (32%); a structurally normal heart was found in 18 patients (53%) and non-specific findings in 2 (6%) (Table 1) (Figure 1). LGE was found in 12 patients (34%), with predominant mid-wall pattern (58%). There was moderate agreement between CMR and TTE final diagnosis (Cohen’s kappa 0.435, p 0.001). CMR determined a change in diagnosis in 14 patients (40%).
{kind=link}
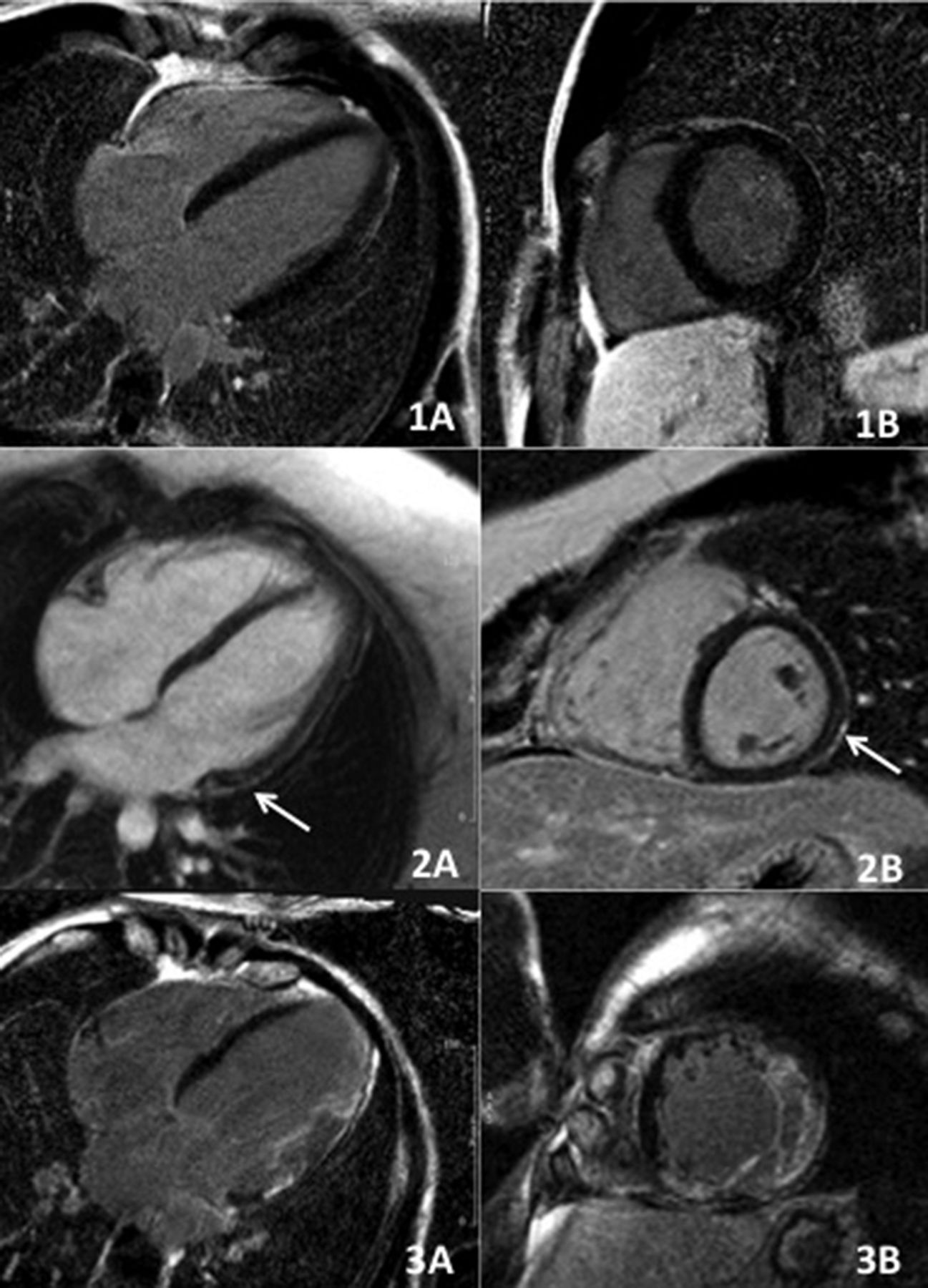
CMR findings. Post-contrast four chamber long-axis (1A) and short-axis (1B) view showing structurally normal heart. Post-contrast four chamber long-axis (2A) and short-axis (2B) view showing epicardial LGE in the basal to mid-cavity lateral wall (white arrow) in a patient with myocarditis. Post-contrast four chamber long-axis (3A) and short-axis (3B) view showing transmural myocardial LGE in the basal to apical lateral wall in a patient with left ventricular non compaction
Conclusions CMR was diagnostic in 94% of young-middle aged patients presenting with high grade AVB. As compared to a multi-parametric pre-CMR diagnosis, CMR led to a change in diagnosis in 40% of patients.
CMR diagnosis