Article Text

Abstract
Introduction Aortic valve regurgitation (AR) and stenosis (AS) increase the workload of the left ventricle (LV), resulting in remodeling of chamber volume and walls that normalise wall stress. Whether functional characteristics of the heart, such as strain (ε), adapt as the heart remodels is unclear. Likewise, we know little about the relationship between changes in volume and strain across the cardiac cycle. This exploratory study utilised a novel technique (ε-volume loops) to establish the contribution of longitudinal (Lε) and transverse strain (Tε) to volume change throughout the cardiac cycle in patients with severe aortic valve disease.
Methods 27 participants with preserved ejection fraction (EF) were included consisting of AR (n = 7), AS (n = 10) and healthy controls (n = 10). Standard transthoracic echocardiography was used to obtain an apical 4 chamber image of the LV. Temporal Lε and Tε values were exported and divided into 5%-time increments. LV volumes were traced at each 5%-time increment. The ε-volume relationship was assessed by 1) the slope of the linear regression line in systole (Sslope) and diastole (Dslope), 2) polynomial equations to derive absolute ε values for% of end diastolic volumes (EDV) in the working physiological range of 10 to 60% EF, 3) a systolic and diastolic exponent (SExp and DExp) as determined by the difference between ε at 10% increments relative to ε at 60% EF and 4) systolic-diastolic coupling (SDcoup) as the difference between systolic and diastolic ε at each 10% increment of EDV (see Figure 1).
Results Patients with AS or AR had significantly lower peak Lε, higher peak Tε and a “flatter” longitudinal Sslope and Dslope compared to controls (see Tables 1 and 2). Following polynomial calculation to specific EDV these differences were partially normalised, suggesting the rate of change is, in part, related to chamber size. Lε but not Tε systolic-diastolic coupling was reduced in AS and AR compared to controls. There was a trend highlighting a higher SExp and DExp (indicating a reduction of ε contribution to volume change in early systole/late diastole) in both patient groups compared to controls for Lε and Tε. There was no significant difference in peak Lε and Tε between AS and AR patients but steeper slope values were observed in AS patients.
Conclusion This exploratory study shows the traditional shift in LV volumes between controls, AS and AR, but also indicates lower peak Lε and higher peak Tε values in AS and AR compared to controls. Although peak Lε or Tε were not different between AS and AR, we reported a distinct relationship between ε and volume between pathologies. Therefore, this novel technique may help to distinguish functional consequences of AS and AR and may have clinical relevance.
Characteristics Lε
Characteristics Tε

A schematic view of the methods used to asses the ε-volume loops. Left: a curve of a typical control ε-volume loop. Right: a curve of the ε-volume loop of a patient with AR

{kind=link}
{kind=link}
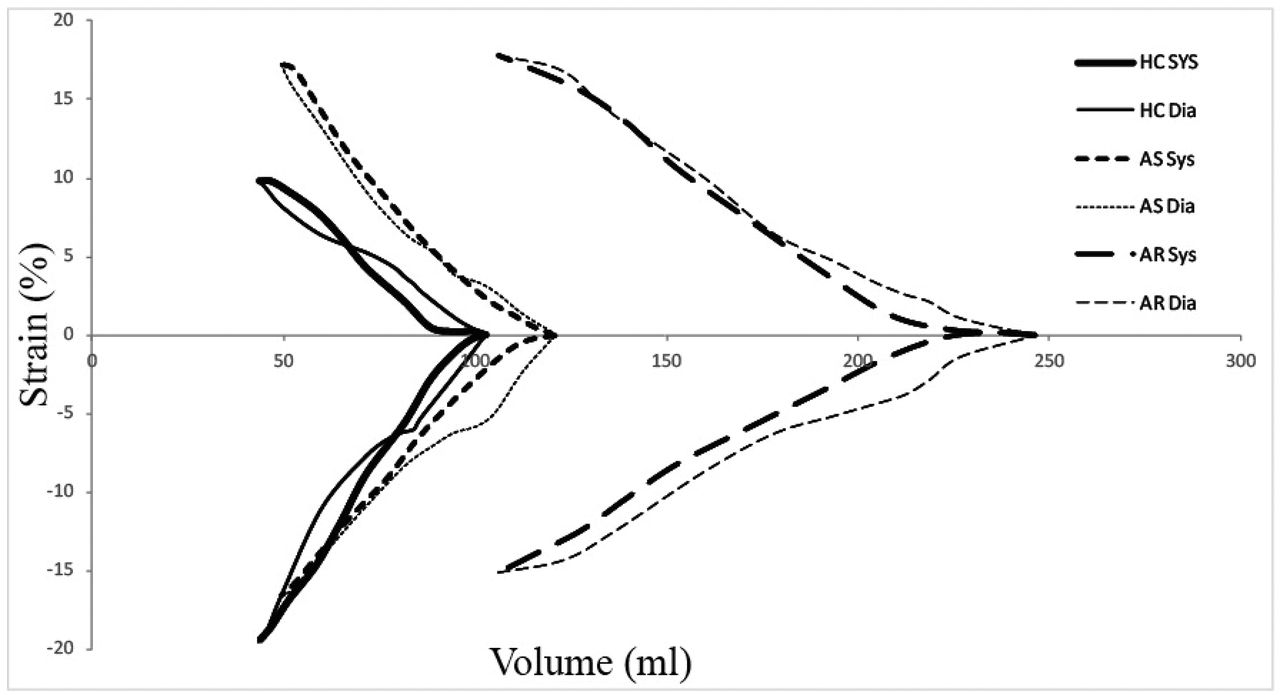
Mean longitudinal and transverse ε-volume loops in controls, AS and AR patients respectively
- echocardiography
- strain-volume loop
- valve disease