Article Text

Abstract
Introduction Significant (>50%) left main stem stenosis (LMS) is found in 4–6% of patients undergoing diagnostic angiography. Unprotected LMS lesions are associated with a poor prognosis and the mortality for non-revascularised disease may be as high as 37% at 3 years. In order to reduce morbidity and mortality associated with delayed treatment, European guidelines recommend that all patients with LMS disease undergo revascularisation within 2 weeks.
Aims We audited all patients in our high-volume tertiary centre that underwent revascularisation by coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI) for significant LMS stenosis during a 6-month period. We sought to investigate timing between coronary angiography and revascularisation for stable and unstable presentations and compare our findings to the international guidelines.
Methods Patients with significant LMS disease observed during invasive coronary angiography (Feb–Aug 2014) were retrospectively identified using the coronary intervention patient-database at the West of Scotland Regional Heart and Lung Centre (Golden Jubilee National Hospital). Data were collected from angiography reports and electronic patient records. Patients who did not undergo revascularisation or who had primary PCI were excluded from the analyses. Patients were considered unstable if the indication for angiography was acute coronary syndrome, including ST-elevation myocardial infarction without primary PCI.
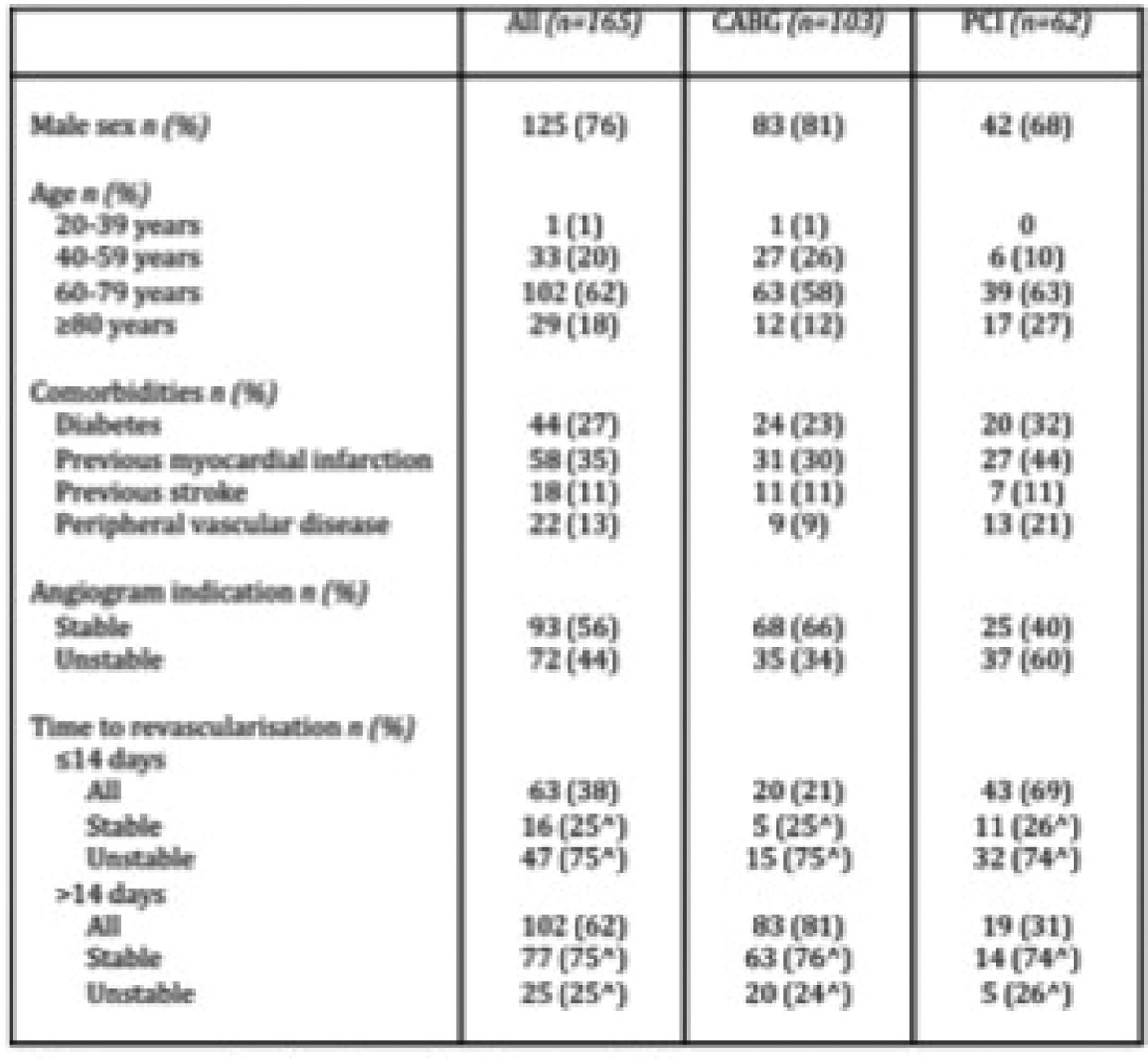
Results 207 patients were found to have significant LMS disease during the audit period, 42 were excluded (not revascularised or primary PCI). A total of 165 patients underwent non-emergency revascularisation. 103/165 (62%) patients were revascularised by CABG. A larger proportion of patients in the PCI group were female, older, had additional comorbidities and were unstable at presentation compared with the CABG group (Table 1). 102/165 (62%) patients waited >14 days for revascularisation. Figure 1 shows the distribution of timing of revascularisation by CABG and PCI, highlighting the stability of patients within each group. 16/93 (17%) stable patients and 47/72 (65%) unstable patients were revascularised within 14 days, with the majority undergoing PCI (43/64, 68%). The main reason for delay >14 days for CABG was the wait for outpatient surgery (Figure 2). In the PCI group waiting >14 days, 5/19 (26%) patients were referred back for PCI after being deemed unsuitable for surgery (Figure 3).

Time to revascularisation stratified by patient stability

Reasons for delay > 14 days for CABG and PCI

{kind=link}
{kind=link}
{kind=link}
Baseline character
Conclusion Huge service developments have been made in recent years to deliver timely revascularisation for patients, particularly those with unstable coronary disease. Despite this, we have found that patients with the highest risk coronary anatomy are experiencing significant delays to revascularisation, particularly by CABG. Further efforts to streamline the pathway to both surgical and percutaneous revascularisation for this patient group are needed.
- Left main stem disease
- Revascularisation
- Timing