Article Text

Abstract
Aims Randomised trials have shown that empiric ICD programming, using long detection times and high detection zones, reduces device therapy in ICD recipients. However, there is less data on its effectiveness in a “real-world” setting, especially secondary prevention patients. Our aim was to evaluate the introduction of a standardised programming protocol in a “real-world” setting of unselected ICD recipients.
Methods We analysed 270 consecutive ICD recipients implanted in a single centre – 135 implanted prior to protocol implementation (Physician-Led group) and 135 after (Standardised group). The protocol included long arrhythmia detection times (30/40 or equivalent) and high rate detection zones (primary prevention lower treatment zone 200 bpm). Programming in the Physician-Led group was at the discretion of the implanter. The primary endpoint was time-to-any therapy (ATP or shocks). Secondary endpoints were time-to-inappropriate therapy and time-to-appropriate therapy. The safety endpoints were syncopal episodes, hospital admissions, and death.
Results At 12 months follow-up, 47 patients had received any ICD therapy (Physician-Led group, n = 31 vs. Standardised group, n = 16). There was a 47% risk reduction in any device therapy (p = 0.04) and an 86% risk reduction in inappropriate therapy (p = 0.009) in the Standardised compared to the Physician-led group. Results were consistent across primary and secondary prevention patients. There were no significant differences in the rates of syncope, hospitalization and death.
Conclusions In unselected patients in a “real-world” setting introduction of a standardised programming protocol, using long detection times and high detection zones, significantly reduces the burden of ICD therapy without an increase in adverse outcomes.

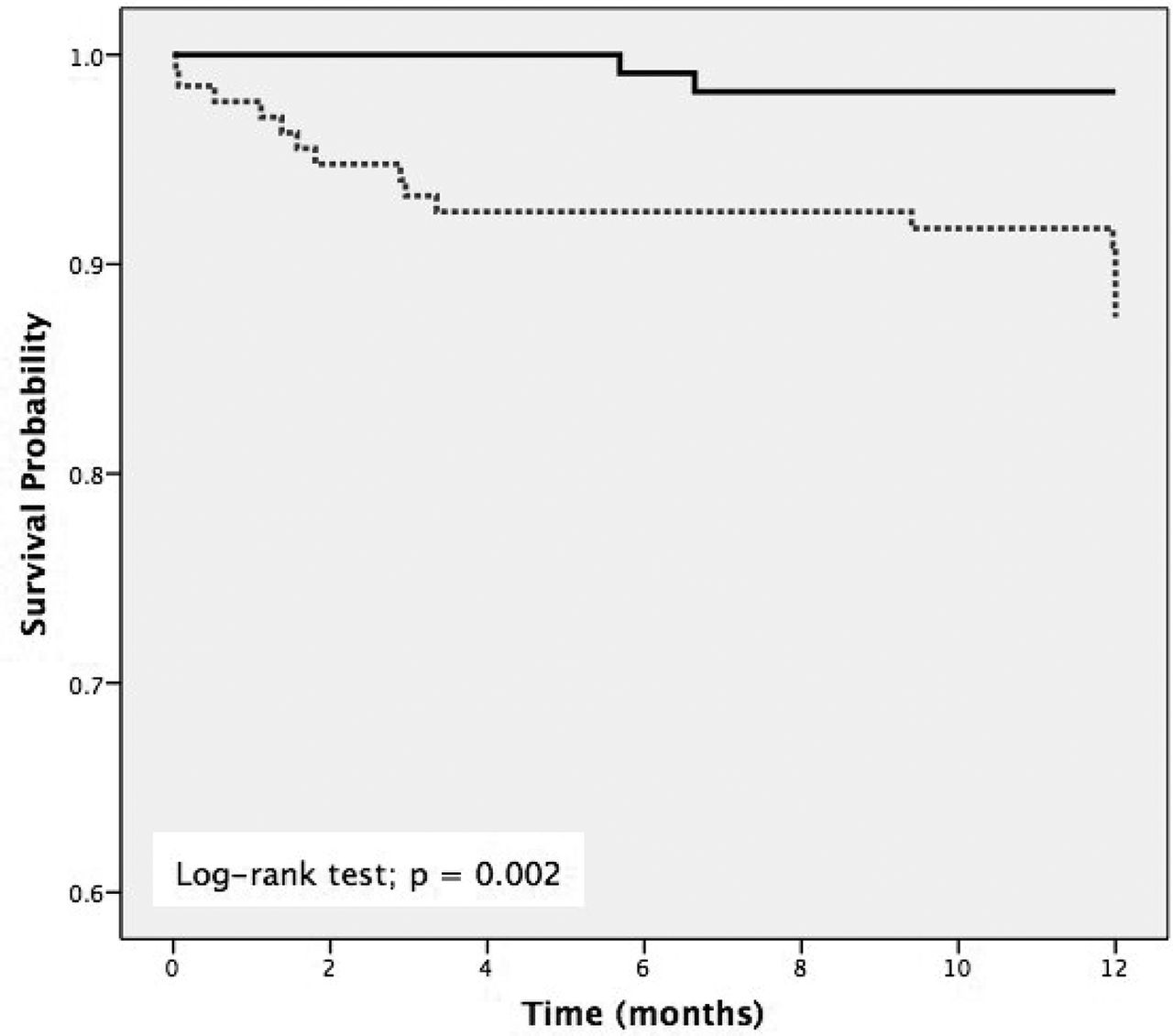
Kaplan-Meier curves for survival from any-therapy. Physician-Led (dotted) vs. Standardised (black)

{kind=link}
{kind=link}
Kaplan-Meier curves for survival from inappropriate therapy. Physician-led (dotted) vs. Standardised (black)
- implantable cardioverter defibrillator
- long detection-time
- programming