Article Text

Abstract
Introduction Cardiac Resynchronisation Therapy (CRT) is an effective therapy for selected patients with heart failure, but is limited in some patients by inability to place the left ventricular (LV) lead via the coronary sinus. We have developed an alternative technique, placing the LV lead endocardially through an interventricular septal puncture. We now report the results of a pilot study assessing this technique, and in addition assessing the optimal endocardial pacing site.
Methods All patients were anticoagulated with INR 2.5–3.5. A superior approach ventricular transseptal puncture using RF energy was performed. We undertook endocardial LV electrical activation mapping. Acute haemodynamic response (AHR) to CRT was assessed at the site of latest electrical activation (LEA), at the site of latest mechanical activation (LMA) as assessed on pre-procedure speckle-tracking echocardiography, and at an empirical lateral position. An active-fixation pacing lead was delivered through the septum to the site with optimal haemodynamics.
Patients were followed up at 6 months with the Packer Clinical Composite Score (CCS) which categorises HF patients as clinically improved or worsened. AHR results were compared with generalised mixed-effects multi-level linear modelling.
Results 18 patients were recruited, 13 with failed transvenous LV lead placement and 5 non-responders to standard CRT with poor LV lead position. Age was 66 ± 12, 83% male, QRSD 156 ± 14 ms, ischaemic 44%, NYHA class 2.9 ± 0.6, EF 28 ± 7%, CHADS-VASc score 3.6 ± 1.4 (all mean+/-SD).
AHR could be assessed in 17 patients; the optimal site was at the LEA in 8, at the LMA in 6 and lateral in 2. Overall there was no significant difference in AHR between the LEA and LMA. Electrical delay >100ms was a significant multivariate predictor of AHR, but placement at the LMA site was not.

Acute haemodynamic response to biventricular pacing at the sites of latest electrical and mechanical activation
The procedure was successful in all and safe with no serious complications, and two wound haematomas.
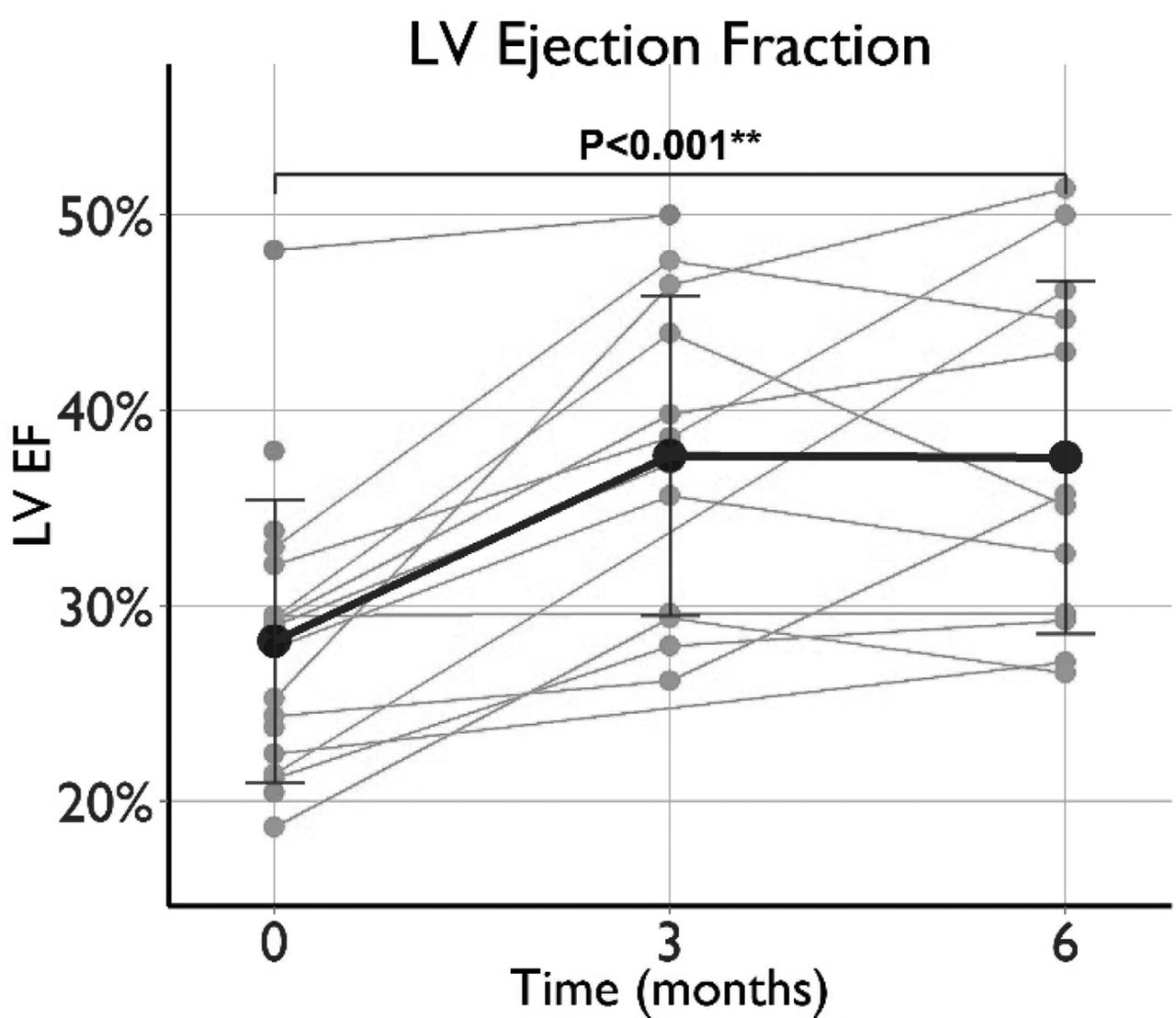
Packer clinical composite score improved at 6 months in 57%, and was worse in 43%. LV ejection fraction improved >5% in 71%, from 28+/-7% to 39+/-9%. 6 min walking distance improved >10% in 75%, from 256+/-128m to 314+/-111m.

{kind=link}
{kind=link}
Response to CRT as assessed by LVEF
One patient suffered a lacunar ischaemic stroke after 5 months with partial neurological recovery, associated with labile INRs. Another died of pneumonia after 3 months.
Conclusions LV endocardial pacing via interventricular septal puncture in patients in whom standard CRT is not possible is similarly effective and durable, with reasonable risks. Optimal pacing sites may need personalisation to the patient, but a lateral position with a long electrical delay is a reasonable empirical site.
- CRT
- Endocardial LV pacing
- transseptal