Article Text

Abstract
Introduction Syncope affects approximately 50% of people in their lifetime. The diagnosis of the underlying cause for syncope is often delayed, inaccurate and cost-inefficient.1 The objective of this study was to evaluate the safety and cost-effectiveness of a novel low-risk syncope day-case assessment unit recently introduced at a DGH.
Methods A retrospective analysis of 50 in-patients admitted with syncope was initially undertaken. Measured variables included length of in-patient admission, waiting time to investigation (24-hour holter and transthoracic echocardiogram), frequency of cardiology review, 30-day re-admission rate with syncope and 90-day mortality rate. The same variables were then assessed prospectively in 50 in-patients referred directly to the syncope clinic. The one-stop assessment unit took place in the local ambulatory care unit (Figure 1) and was led by acute medical physicians; with access to transthoracic echocardiography and continuous ECG monitoring which were all performed on the same day. Patients were referred for same-day specialist review as appropriate. All 100 patients were deemed low risk as defined by the San-Francisco Syncope Rule.3 Patients investigated for conditions other than syncope were excluded. Student’s t-test and chi-squared tests were used to compare continuous and categorical data respectively.

Based on : European Society of Cardiology’s Guidelines for the diagnosis and management of syncope (version 2009)
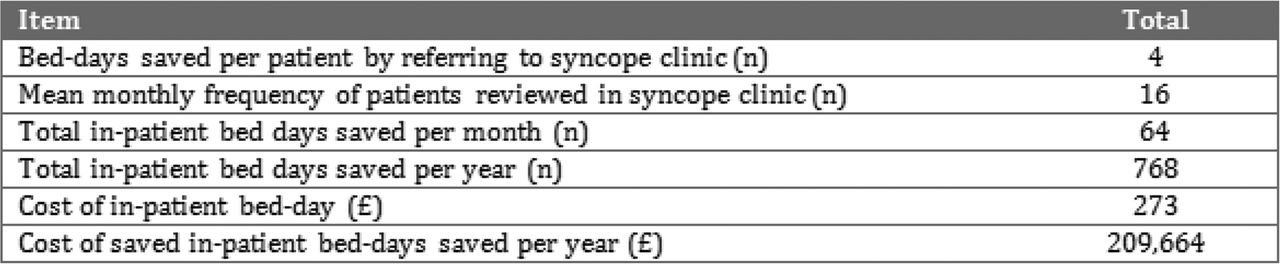
Results The median length of admission for patients remaining in hospital for assessment was 4 days compared to 1 day for those referred to the syncope assessment unit (p < 0.05). The median waiting time from discharge for a syncope unit appointment was 3 days. 32% of the patients referred to the syncope clinic were reviewed or discussed with a cardiologist. This figure was higher (46%) for those patients remaining in hospital for assessment although not statistically significant (p = 0.151). There was no significant difference in 30-day readmission rate with syncope or 90-day mortality rate between the two (p > 0.05). 93 patients were reviewed in the syncope clinic over the first 6 months (16/month). With an in-patient bed-day costing £273, referral of patients to the syncope clinic at this rate would save £17,472 per month and £209,664 per year (Tables 1 and 2).

Summary of patient variables
{kind=link}
{kind=link}
{kind=link}
Summary of projected cost data
Conclusions The introduction of a novel low-risk syncope assessment unit promotes early discharge from hospital with prompt outpatient medical review and shorter waiting times for diagnostic investigations. Our data suggests this is both cost-effective and safe with improved patient care.
References
Transient loss of consciousness (‘blackouts’) in over 16s. NICE guidelines [CG109] Published date: August 2010
Kapoor WN, Karpf M, Wieand S, Peterson JR, Levey GS. A prospective evaluation and follow-up of patients with sycope. N Engl J Med. 1983;309:197-–203
Quinn JV, Stiell IG, McDermott DA, Sellers KL, Kohn MA, Wells GA. Derivation of the San Francisco Syncope Rule to predict patients with short-term serious outcomes. Ann Emerg Med. 2004;43:224–32
- AECU
- Syncope
- Ambulatory