Article Text

Abstract
Background Venous thromboembolism (VTE) is the most common preventable cause of death with safe and effective prevention measures available. Inpatients at high risk for VTE often fail to be provided prophylaxis despite clear guidelines and this mismatch between VTE prophylaxis and thromboembolic risk is a major issue for clinicians. We sought to clarify compliance of practice with the NICE quality standard and to assess accuracy of the Commissioning for Quality and Innovation (CQUIN) VTE form.
Methods A point prevalence study was performed involving a comprehensive review of 100 consecutive patients at Barnet Hospital. We assessed compliance against the NICE guideline 92 by ensuring appropriate assessment of VTE and bleeding risk, clarifying that those where the VTE risk outweighs the bleeding risk are offered prophylaxis. We also assessed the accuracy of VTE risk assessment form completion using validated bleeding risk (HASBLED) and VTE risk (Wells) scores. We implemented technical improvements in the VTE risk assessment form; medical education through mandatory completion of VTE eLearning modules; and involvement of the MDT through grand round discussions. Following implementation, a reaudit of 50 patients was performed.
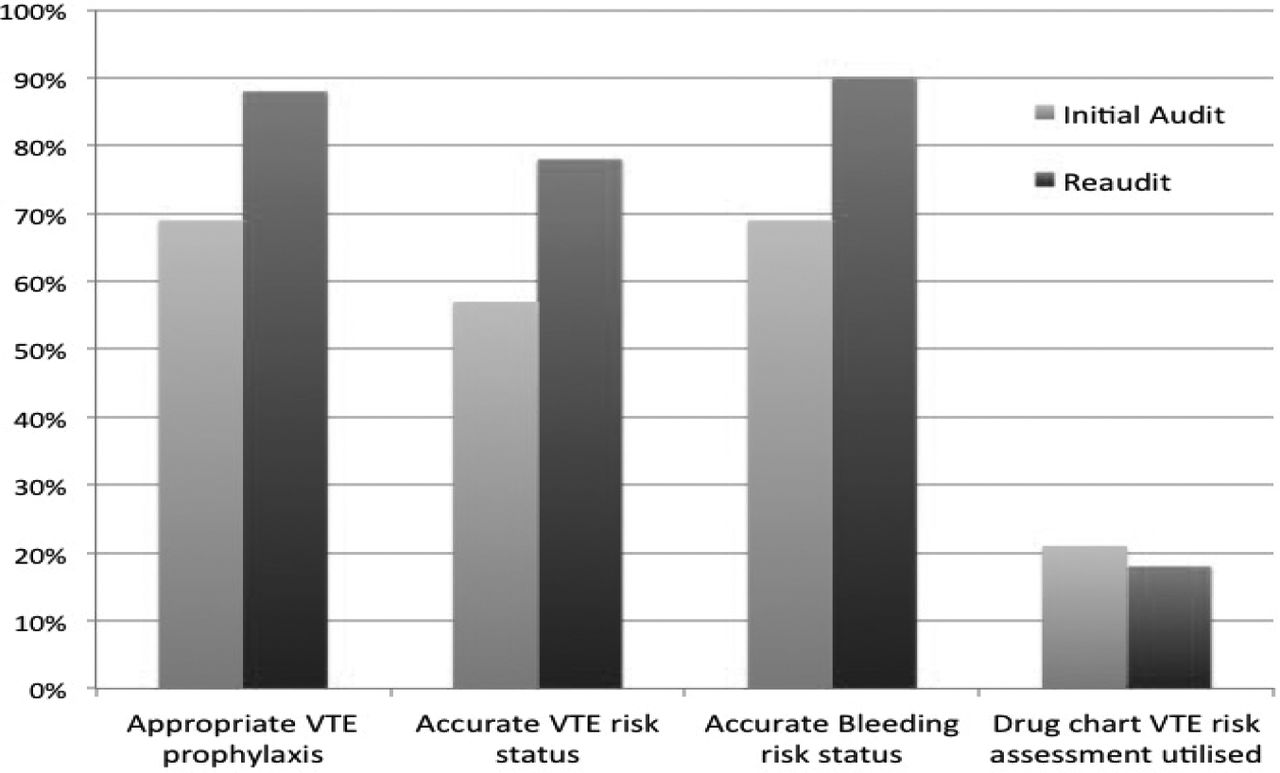
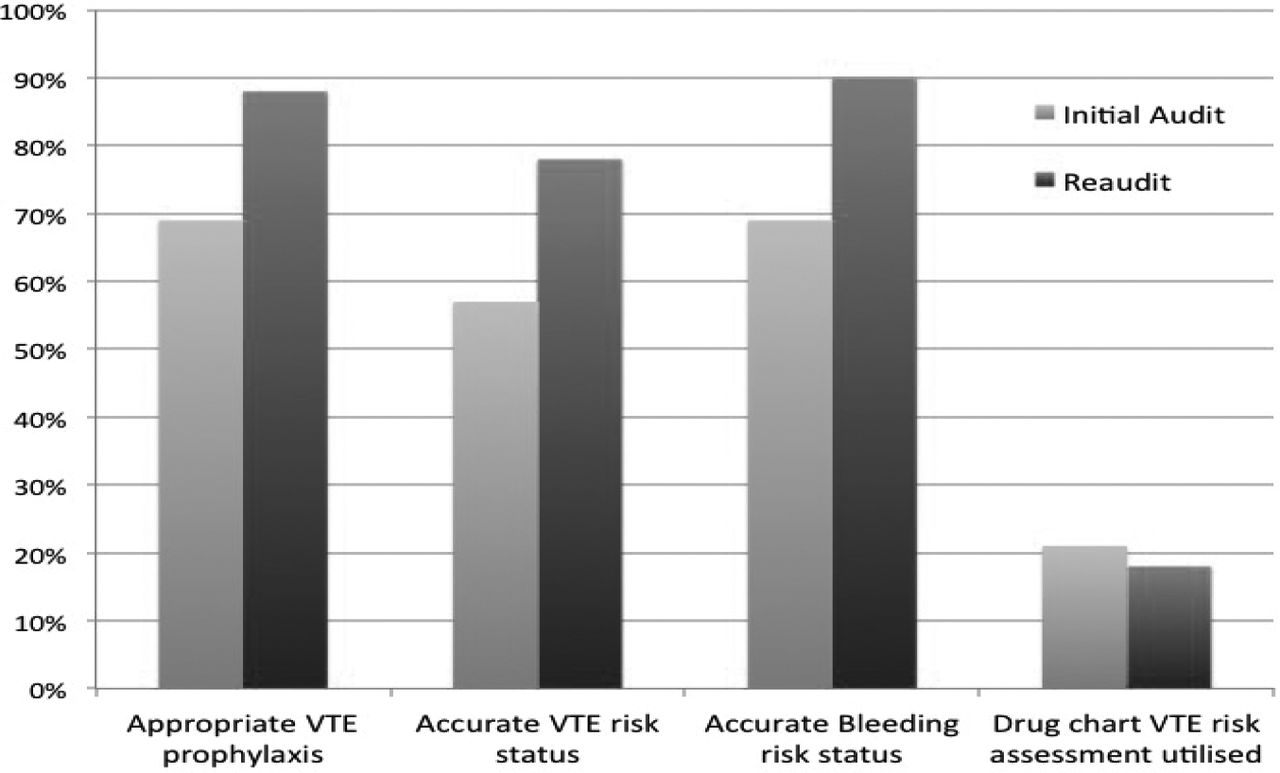
Results In 100 patients assessed, mean age was 71 years, 55 were male, with mean weight 74.8kg; see Table 1. Based on the drug chart, VTE prophylaxis was appropriately offered in 69% of patients; see Figure 1. The VTE risk assessment form was accurately completed in 57% for VTE risk status, in 69% for bleeding risk, and in 69% for VTE prophylaxis prescribed. After implementations, the reaudit revealed VTE prophylaxis was appropriate in 88%, VTE risk assessment form was accurate in 78% for VTE risk status, 90% for bleeding risk, and 89% for VTE prophylaxis prescribed. The section of the drug chart devoted to VTE risk assessment was poorly utilised; 21% in the initial audit and 18% in the reaudit.
Characteristics of the participants by initial audit and reaudit
{kind=link}
Conclusion Whilst single centre and modest in size, this robust, complete audit demonstrated compliance with VTE prophylaxis guidelines was poor, for both risk assessment and appropriate prescribing. Technical improvements to the VTE form, educating trainees and involving the MDT significantly improved compliance with guidelines. Future work is required to overcome accuracy issues of form completion ensuring patients receive optimal care.
- Venous Thromboembolism
- Audit
- Quality Improvement