Article Text

Abstract
Introduction Current pharmacodynamic (PD) data suggest reduced antiplatelet effect in ST-Elevation myocardial infarction (STEMI) of prasugrel and ticagrelor. We sought to investigate the early PD effect of prasugrel and ticagrelor administered in two patient groups: those admitted with STEMI and a cohort admitted with NSTEMI/unstable angina (UA).
Methods P2Y12 inhibitor naïve patients presenting with STEMI or NSTEMI/UA were assessed for inclusion. All patients provided informed consent. All received aspirin (300mg) and loading dose of either prasugrel (60mg) or ticagrelor (180mg) in a non-randomised fashion. Platelet reactivity was measured using VerifyNow assay at 20 min, 1 and 4 h post loading. Results are expressed a P2Y12 reaction units (PRU). PRU≥208 indicates a sub optimal antiplatelet response. PRU over time was tested between groups using 2 way ANOVA, P < 0.05 was considered significant.
Results A total of 58 patients were enrolled (30 STEMI, and 28 NSTEMI/UA Table 1).
Baseline characteristics
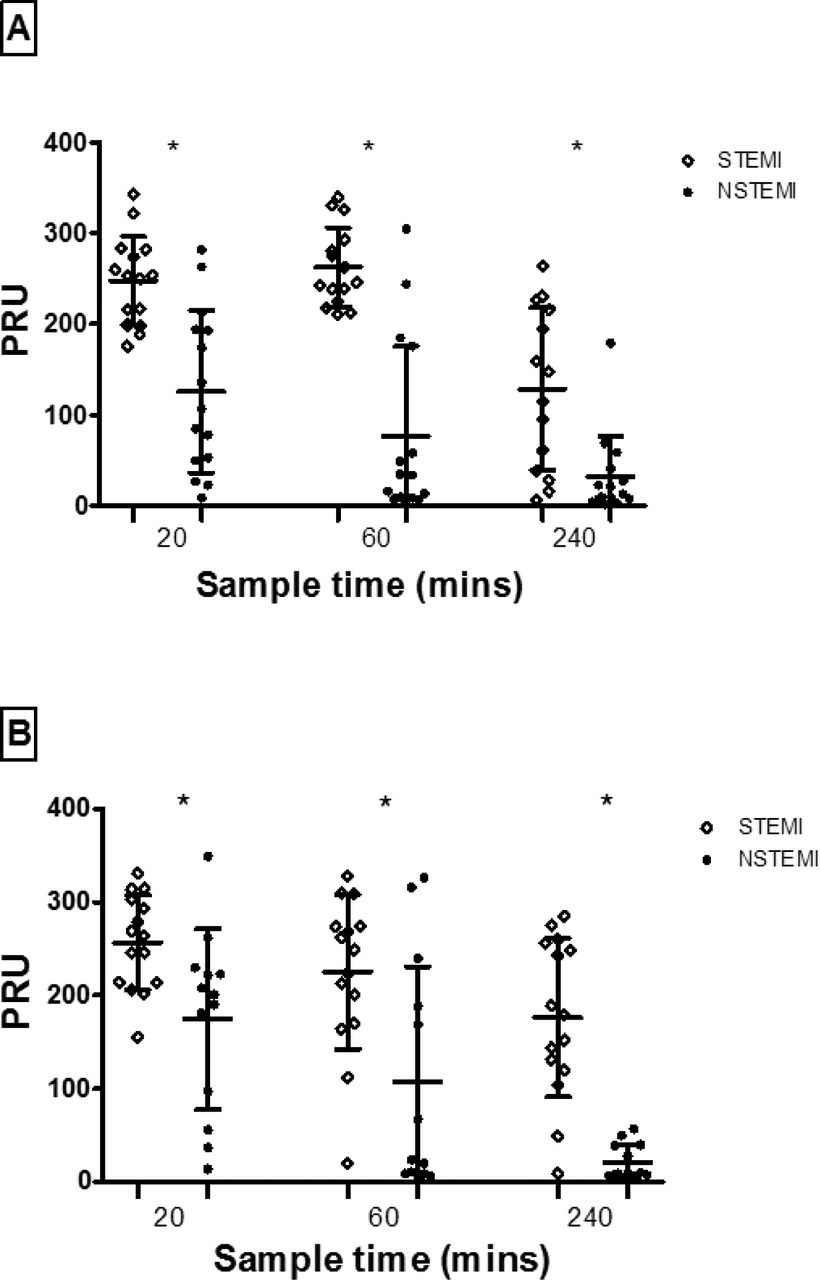
Results are shown in Fig 1. In the STEMI patients there was little effect of either agent at 20 min post loading (prasugrel PRU 247 + 48.8, ticagrelor PRU 256 + 50.8) with a limited effect at 1 h and persisting attenuated results at 4 h. In the NSTEMI group however there was a marked and rapid antiplatelet effect of both agents at all time points. Over time there was a significant difference between the effect of both prasugrel ( P < 0.001) and ticagrelor ( P < 0.001) in STEMI patients vs NSTEMI patients. There was no significant difference in the effect of ticagrelor vs prasugrel over time in either STEMI or NSTEMI/UA.

{kind=link}
The degree of inhibition of platelet reactivity (expressed as PRU) over time following the administration of prasugrel (A) and ticagrelor (B) in STEMI and NSTEMI patients. PRU = P2Y12 reactivity units
Conclusion Prasugrel and ticagrelor in the context of STEMI do not provide adequate P2Y12 inhibition at reperfusion and the first hour post loading when compared to patients with NSTEMI/UA.
- P2Y12 inhbitors
- Platelet Function
- ACS