Article Text

Abstract
Introduction Atrial fibrillation (AF) is associated with increased risk of heart failure and premature death, and is often resistant to treatment. Animal models of pacing-induced AF indicate that AF-induced endothelial dysfunction, impaired coronary reserve, and myocardial remodelling are important in arrhythmia maintenance. However, human AF may reflect a subclinical cardiomyopathy, which persists after sinus rhythm (SR) restoration and provides a substrate for AF recurrence. To test this hypothesis, we investigated the effect of restoring SR by catheter ablation on left ventricular (LV) function and energetics.
Methods 96 subjects were recruited: 53 patients referred for AF ablation, 18 controls in SR matched to patients for age, sex and BMI, and 25 healthy controls (Table 1). Patients had symptomatic paroxysmal (n = 27) or persistent (n = 26) ‘lone’ AF (without coronary artery disease, valvular disease, diabetes, uncontrolled hypertension or inadequate ventricular rate-control). Cardiac magnetic resonance (MR) short axis cines were analysed by a blinded investigator to calculate LV volumes and ejection fraction (EF). 31Phosphorus MR spectroscopy determined myocardial energetics (ratio of phosphocreatine to ATP [PCr/ATP]). Patients were scanned pre-ablation, early post-ablation (~20 h, n = 48) and late post-ablation (~7 months, n = 41).
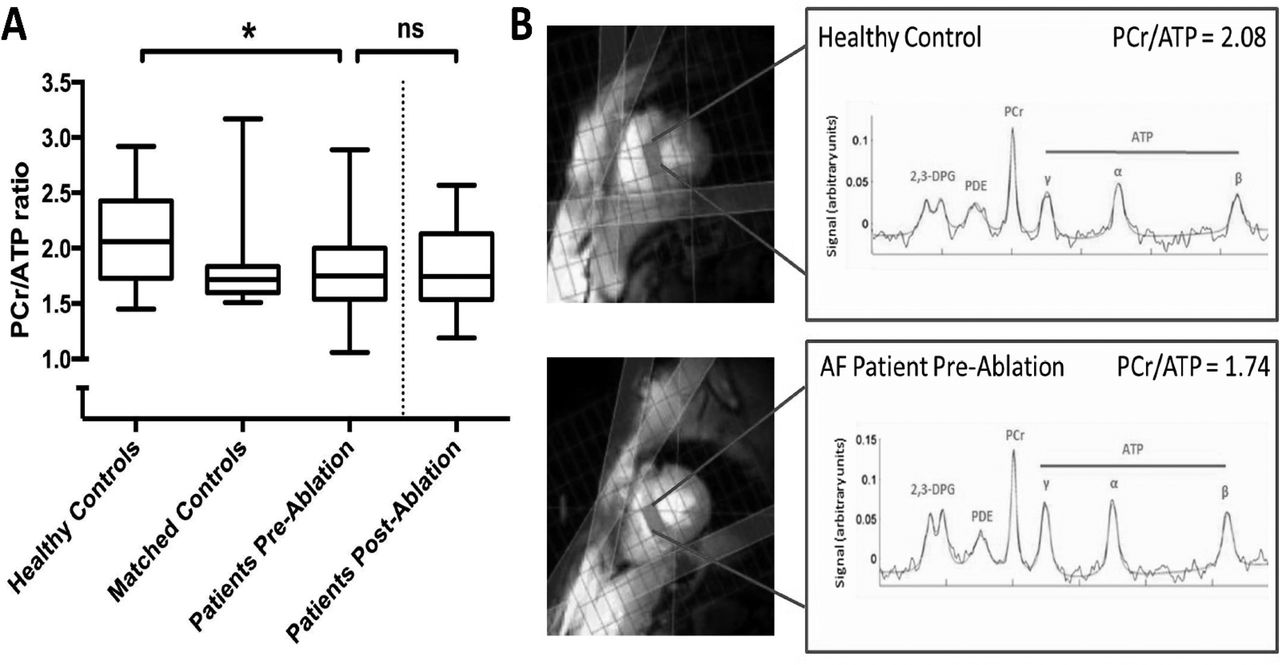
Results In patients pre-ablation, LVEF was significantly lower than in matched and healthy controls (59 +/-± 10 vs 69 ± 6 and 68 ± 5% respectively, p < 0.001). Myocardial energetics was also impaired compared to healthy controls (median PCr/ATP 1.75 vs 2.06, p = 0.04) but not matched controls (median PCr/ATP 1.72, p=ns; Figure 1). In patients, those scanned in AF had lower LVEF (54 ± 10 vs 66 ± 7%, p < 0.001), but not energetics (median PCr/ATP 1.74 vs 1.84, p = 0.66), compared to those scanned in SR.
Early post-ablation, recovery of SR from AF was associated with significant improvement in LVEF compared to patients in SR during both the pre-ablation and early post-ablation scans (+7 ± 10 vs -−0.2 ± 7%, p = 0.02). Late post-ablation, LVEF in patients (63 ± 8%) remained impaired compared to matched controls (p = 0.012). Myocardial energetics were also unchanged post-ablation (median PCr/ATP 1.74 vs 1.82, p = 0.39), irrespective of ablation success.
Conclusions Even ‘lone’ AF is associated with LV dysfunction and impaired myocardial energetics. LV function partially improves with recovery of SR early post-ablation, indicating an acute haemodynamic effect. However, ablation fails to normalise LV function or reverse energetic impairment at later follow-up. These novel findings suggest that human AF may be the consequence (rather than the cause) of an occult cardiomyopathic process that develops with ageing and risk factors. Comprehensive therapeutic strategies that target and reverse this phenotype may reduce AF recurrence and improve clinical outcomes.

{kind=link}
(A) Myocardial energetics is impaired in patients compared to healthy controls, but not matched controls. (B) Representative 31P spectra from a mid-ventricular septal voxel in a healthy control (PCr/ATP ratio 2.08) and an AF patient pre-ablation (PCr/ATP ratio 1.74). PCr/ATP = ratio of area under phosphocreatine peak to average area under the three ATP peaks. Kruskal-Wallis test with post-hoc pairwise comparison adjusted for multiple testing (healthy controls, matched controls, patients pre-ablation) and separate related-samples Wilcoxon Signed Rank Test (patients pre-ablation and patients post-ablation). *indicates p < 0.05; centre line indicates median, box indicates interquartile range and error bars indicate range
- Atrial fibrillation
- Ventricular function
- Magnetic resonance