Article Text

Abstract
Introduction Chronic Kidney Disease (CKD) is a risk factor for contrast induced nephropathy (CIN), defined as an increase in serum creatinine of >25% from baseline or a delta rise of >26.5µmol/L within 48 hours. Early diagnosis of acute kidney injury (AKI) associated with CIN requires validated novel biomarkers.
Methods A prospective observation study of 301 consecutive CKD patients undergoing elective invasive coronary angiography was performed. Low-osmolar contrast was standard. Demographics and Mehran risk score were recorded. Samples for plasma neutrophil gelatinase-associated lipocalin (NGAL), serum liver fatty acid-binding protein (L-FABP), serum kidney injury marker 1 (KIM-1), serum interleukin 18 (IL-18) and serum creatinine were taken at 0, 1, 2, 4, 6 and 48 hours post contrast. Urinary NGAL and urinary cystatin C (CysC) were collected at 0, 6 and 48 hours. Incidence of major adverse clinical events (MACE); acute myocardial infarction, heart failure hospitalisation, stroke and death were recorded at 1 year.
Results CIN occurred in 28 (9.3%) patients and were independently associated with older age, diabetes, higher Mehran score, larger contrast volume and anaemia (p < 0.05). Logistic regression analysis showed diabetes, CKD stage and GFR to be most predictive of CIN. The predictive power of plasma NGAL was greatest at 6 hours with median levels of 1,337 ng/ml in CIN patients compared with 931 ng/ml in non-CIN patients (p = 0.002, AUC 0.71, sensitivity 75.0%, specificity 96.1%, OR 2.86), see Figure 1 and Table 1. L-FABP performed best at 4 hours with median levels of 10.7 ng/ml in CIN patients compared with 6.2 ng/ml in non-CIN patients, p = 0.001, AUC 0.69, sensitivity 42.3%, specificity 90.2%, OR 6.75, Figure 1 and Table 1. Median urinary NGAL was higher only after 48 hours, 487 ng/ml in CIN patients versus 155 ng/ml in non-CIN patients, p = 0.008, AUC 0.63. CysC, IL-18 and KIM-1 were not predictive at any time-point (p > 0.05). A Mehran score ≥ 10 performed prior to procedure achieved an AUC of 0.65, p = 0.006. MACE occurred in 7 (25.0%) CIN patients but only 17 (6.2%) non-CIN patients (p < 0.001). CIN cases also had considerably higher mortality (10.7% compared to 3.3%, p = 0.037). Exploratory analysis showed that the combination of Mehran score >10, 6 hr NGAL and 4 hr L-FABP improved specificity to 96.7%. Figure 2 highlights how biomarkers could be used to identify CIN early and facilitate timely therapeutic intervention to reduce morbidity and mortality.
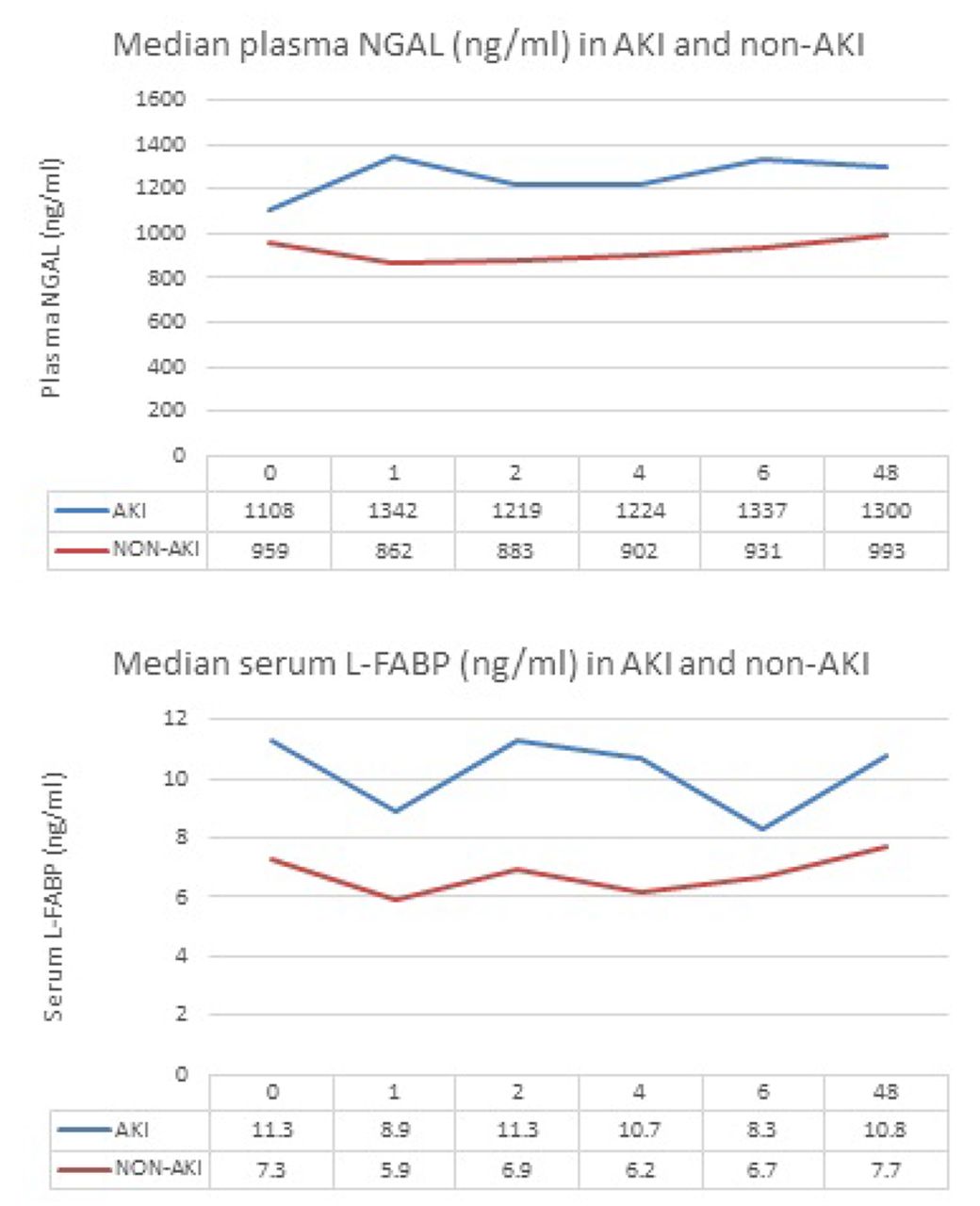
Median plasma NGAL (ng/ml) and serum L-FABP (ng/ml) in AKI and non AKI
Summary of NGAL (ng/ml) and L-FABP (ng/ml) in AKI and non-AKI patients

{kind=link}
{kind=link}
Proposed patient pathways
Conclusions/implications Mehran risk score, 6 hour plasma NGAL and 4 hour serum L-FABP performed best at early CIN prediction. CIN patients were four times more likely to develop MACE and had a trebling of mortality risk at 1 year. The implications of our results, translated to the design of safer elective coronary intervention services able to more efficiently manage the increasing volume of contrast studies, should be a key health priority for providers of cardiac and renal services.