Article Text

Statistics from Altmetric.com
Although at least 80% of cardiovascular disease (CVD) is potentially preventable by the elimination of health risk behaviours, implementation of effective, large scale and sustainable CVD prevention programs is still a challenge. In this issue of Heart, Connolly et al 1 describe an experience in which patients at high risk of or with established CVD underwent a 12 week community-based nurse-led prevention programme called My Action (figure 1) which included lifestyle and risk factor management, prescription of medication and weekly exercise and education sessions. The programme is in accordance to recent British recommendations that CVD should be managed as a family of diseases in the community. The study was conducted in Westminster, a culturally and socioeconomically diverse borough in central London. Over a 6 year period, 3232 patients attended an initial assessment, 63% were male and 48% belonged to black and minority ethnic groups; 56% attended an end of programme assessment and 33% a 1 year assessment. The results were very encouraging in both high risk and CVD patients, with improvement in goals related to unhealthy habits and increase in proportions of patients achieving their BP (CVD +15.4%; high-risk +25%) and LDL-cholesterol targets (CVD +6%, high-risk +23%), as well increase of use of statins and antihypertensive medications in high-risk subjects and improvements in depression scores and quality of life measures. Most improvements were maintained after 1 year.

The MyAction prevention programme.1
In the companion editorial, Dr Ofori2 discusses the key principles of a modern integrated preventive cardiology programme (table 1), saying that ‘a paradigm shift from provider- or disease-centred care to person-centred care is required’. For Dr. Ofori, the MyAction, a nurse-led multidisciplinary prevention programme, exemplifies the future direction of modern preventive cardiology and a viable way to realise the aims of reducing CVD events.
Key principles of a modern integrated preventive cardiology programme2
Management of anticoagulation for prevention of embolic events in patients with atrial fibrillation (AF) and chronic kidney disease (CKD) is especially challenging. In a retrospective analysis of almost 124 thousand patients with newly diagnosed AF, there was an inverse relationship between CKD severity and use of vitamin K antagonist anticoagulation.3 In addition, the time in therapeutic range was lower in those with more severe CKD; only 21% of patients on dialysis were in therapeutic range at least 60% of the time. (figure 2) The authors suggest that the variability in using Vitamin K antagonist therapy in CKD patients has implications for consideration of alternative therapeutic approaches in this patient population.

Percent time in therapeutic international normalised ratio (INR) range, stratified by year of warfarin use.3
In an editorial, Black-Maier and Piccini4 remind us that about 20% of patients with end-stage renal disease have AF and an even higher risk of stroke than predicted by conventional risk factors. Management is complicated by ‘alterations in haemostasis that predispose patients to haemorrhagic (platelet α granule depletion, reduced endothelial cell adhesion molecule expression) and thrombotic (increased circulating fibrinogen) complications, limiting extrapolation of data from patients with normal renal function.’ They then discuss the potential options of direct oral anticoagulants (DOACs) in patients with mild to moderate CKD or left atrial appendage occlusion in dialysis patients but caution that currently there are no ideal options.
A different clinical concern in prevention of embolic events in adults with atrial fibrillation is the potential risk of liver injury with DOACs. In a database analysis of almost 114 thousand patients with atrial fibrillation with a median follow-up of 12 months, there were 960 hospitalisation for liver injury.5 The estimated rates of liver injury per 1000 person-years ranged from 4.0 with dabigatran to 9.0 with warfarin. After multivariable adjustment, hospitalisation rates for liver injury compared with warfarin were 0.57 (0.46 to 0.71) for dabigatran, 0.88 (0.75 to 1.03) for rivaroxaban and 0.70 (0.50 to 0.97) for apixaban. (figure 3) Clinical factors that increased the risk of liver injury included prior liver, gallbladder or kidney disease, cancer, anaemia, heart failure and alcoholism.
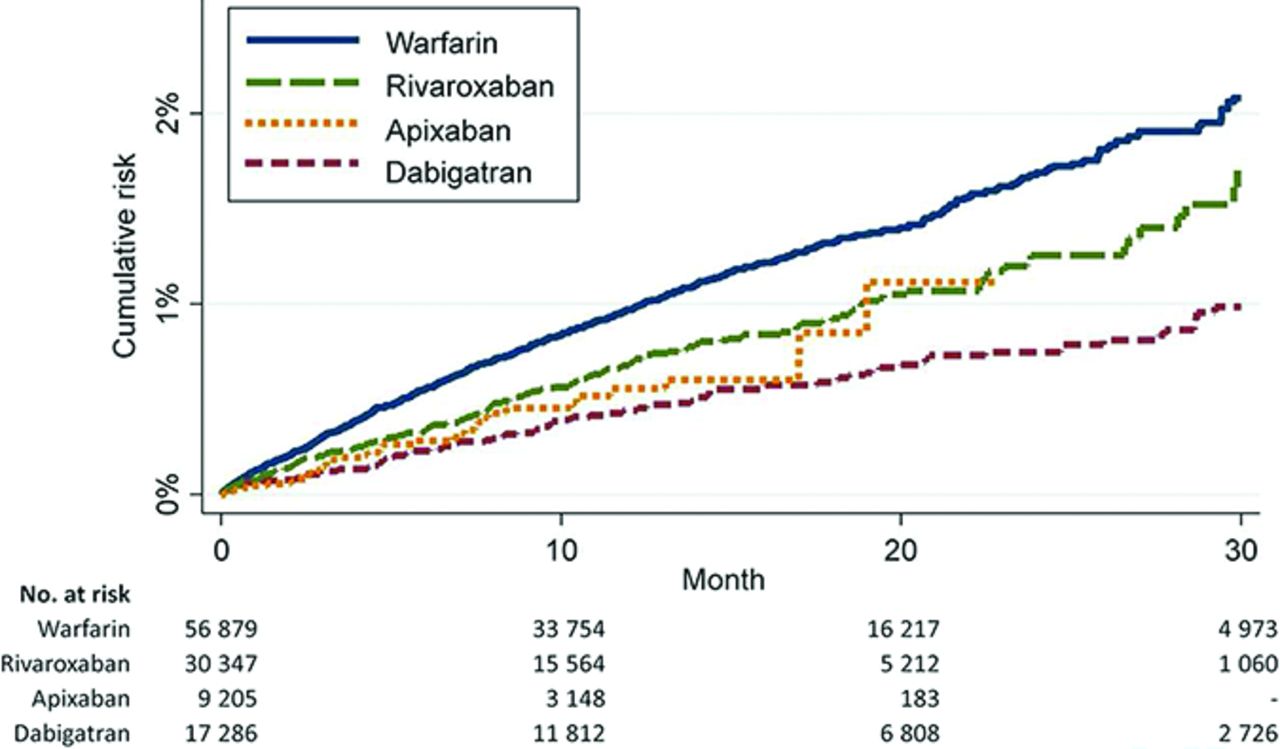
Cumulative risk of liver injury hospitalisation by type of oral anticoagulant, MarketScan databases, 2011–2014. Follow-up truncated at 30 months.5
Potpara and Lip6 put this data in context in their commentary on drug-induced liver injury (DILI) which has been reported with over 1000 medications or herbal products and has an estimated annual incidence of 1–1.5 per 1000 to 10 000 exposed people but accounts for about 10% of all acute hepatitis cases. Clinical trials are unlikely to detect rare events, such as liver injury, so these complications more often are evidence on meta-analyses or large post-market databases, such as the one reported in this issue of Heart . They go on to provide specific clinical guidance on choice of anticoagulation medications in adults with concurrent liver disease. They conclude: ‘Clinical vigilance and regular follow-up of NOACs users are needed to prevent severe, potentially deleterious DILI, but there is no compelling evidence that any particular NOAC should be denied to most patients with AF at risk of stroke only to avoid a rare event such as DILI. However, more data are needed to inform optimal use of NOACs in patients with AF with liver dysfunction.’
The Education in Heart article in this issue, summarises the data on optimal duration of dual antiplatelet therapy after coronary stenting for an acute coronary syndrome and provide a simple proposed algorithm (figure 4).7

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proposed algorithm for optimal duration of DAPT. CAD, coronary artery disease; DES, drug-eluting stent; PAD, peripheral artery disease; ST, stent thrombosis; DAPT, dual antiplatelet therapy.7
A state-of-the-art review article by Sperry and Tang8 discusses the genetics of amyloid heart disease. Amyloid heart disease offers a clinical model in which gene therapy with small interfering RNA and antisense oligonucleotides might stop the abnormal protein production that leads to clinical cardiac dysfunction.
Footnotes
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.