Article Text

Statistics from Altmetric.com
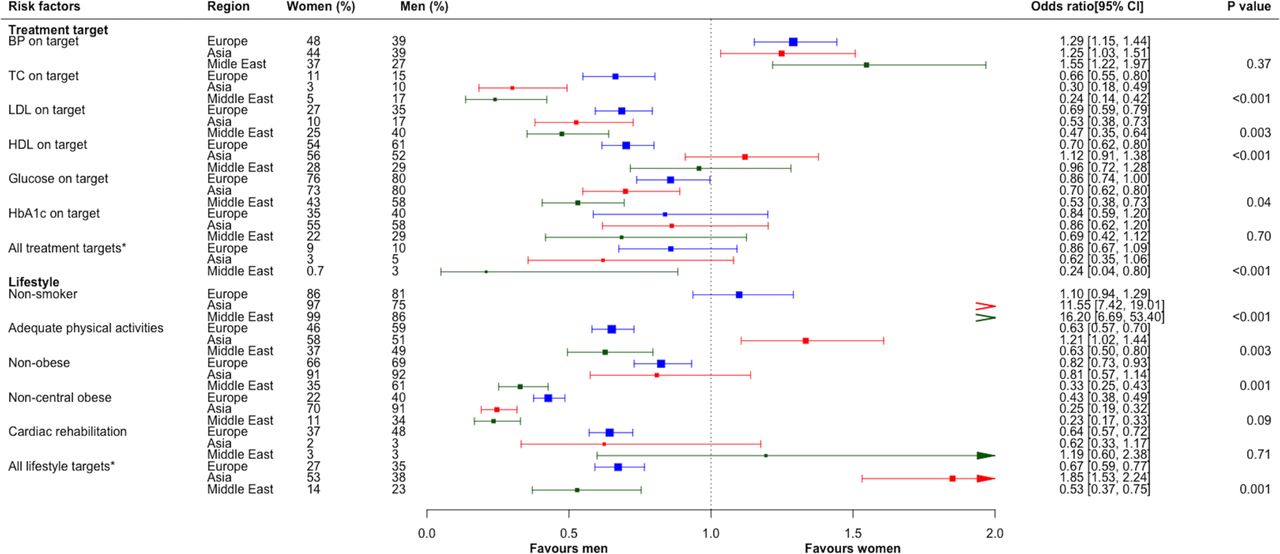
Cardiovascular disease is the leading cause of death in women worldwide. Despite the known sex differences in clinical presentation, management and outcomes of patients with coronary heart disease (CHD), possible differences in primary and secondary prevention have received less attention. In this issue of Heart , Zhao and colleagues1 investigated sex differences in cardiovascular risk factor management in over 10 thousand patients (29% women) from Europe, Asia and the Middle East. Compared with men, women had better blood pressure control and were more likely to be non-smokers. However, women were less likely to achieve medication targets for total cholesterol, low density lipoprotein cholesterol or serum glucose levels. In addition, women were more often obese and less physically active than men. Overall, lifestyle targets for cardiovascular risk reduction did not differ between women and men but women were about 25% less likely to achieve medication treatment targets with marked geographic sex disparities for both lifestyle and medication treatment targets (figure 1).

Age-adjusted sex differences on treatment targets and lifestyle factors management, stratified by region. Target blood pressure (BP) was defined as BP <140/90 mmHg in those without diabetes or <140/80 mmHg in those with diabetes. The target for total cholesterol (TC), low-density lipoprotein (LDL) cholesterol and high-density lipoprotein (HDL) cholesterol levels were defined as <3 mmol/L, <1.8 mmol/L, and >1.0 mmol/L for men and >1.2 mmol/L for women, respectively. Target glucose was defined as <7 mmol/L. Information on glycated haemoglobin (HbA1c) was only collected from patients with diabetes and its target was defined as <7%. *Achieving all three medical targets (BP on target, LDL on target, and glucose/HbA1c on target) was defined as ‘All treatment targets’. Obesity was defined as a body mass index (BMI) ≥30 kg/m2 and central obesity was defined as waist circumference ≥88 cm for women and ≥102 cm for men. Smoking status was current smoker and non-smoker. Adequate physical activity level was defined as moderate or vigorous physical activity for at least 30 min three or more times a week. *Reaching all three lifestyle targets (non-smoker, adequate physical activities, and nonobesity) was defined as ‘All lifestyle targets’. Odds ratios (95% CI) presented as women versus men; p values are for interaction between subgroups.
In the accompanying editorial, Al Badri and colleagues2 comment that “The failure to receive evidence-based therapies in women is sadly a recurrent theme increasingly documented worldwide”. They conclude that: “Knowledge gaps remain, which can be addressed by careful phenotyping of the increasingly available digital medical records and ambulatory monitoring technology, including proteomics, metabolomics, and genomics. Investigation addressing if large sex differences in risk factor management are due to lower treatment of women/higher treatment of men (USA and Europe), vs if lower sex differences are due to lower treatment of both women and men (Asia and Middle East). The need for country and region-specific IHD data stratified by sex is needed to optimise personalised medicine” (figure 2).

Sex-specific and gender-specific medicine is the most ready-for-translation approach among the genomic, proteomic, and metabolomic personalised medicine approaches.
In a French study of 9012 men and women, age 50 to 75 years of age, Simon and colleagues3 found that 14.77% of women but only 6.84% of men met at least 5 of the seven metrics defining ideal cardiovascular health. These metrics include ideal values for body mass index, smoking status, blood pressure, blood total cholesterol, blood glucose and physical activity. Women were slightly older, less educated, more often depressed and more deprived than men; after adjustment for these factors women were four times more often in ideal cardiovascular heart than men (OR 4.01, 95% CI 3.42 to 4.69). These findings parallel the findings in Europeans in the study by Zhao and colleagues1 showing that risk factors for ischaemic disease are lower in European women compared with men; the exception is ideal cholesterol levels, which were less often achieved in women. The authors conclude “it appears that behavioural cardiovascular heart needs to be particularly promoted in men, at least after 50 years of age”. However, in my view the most remarkable finding in this study is how few women or men were in ideal cardiovascular health, only 7% to 15% overall. Clearly, our goal should be to improve risk factor reduction in both men and women, particularly lifestyle factors such as an ideal body mass index and higher levels of physical activity.
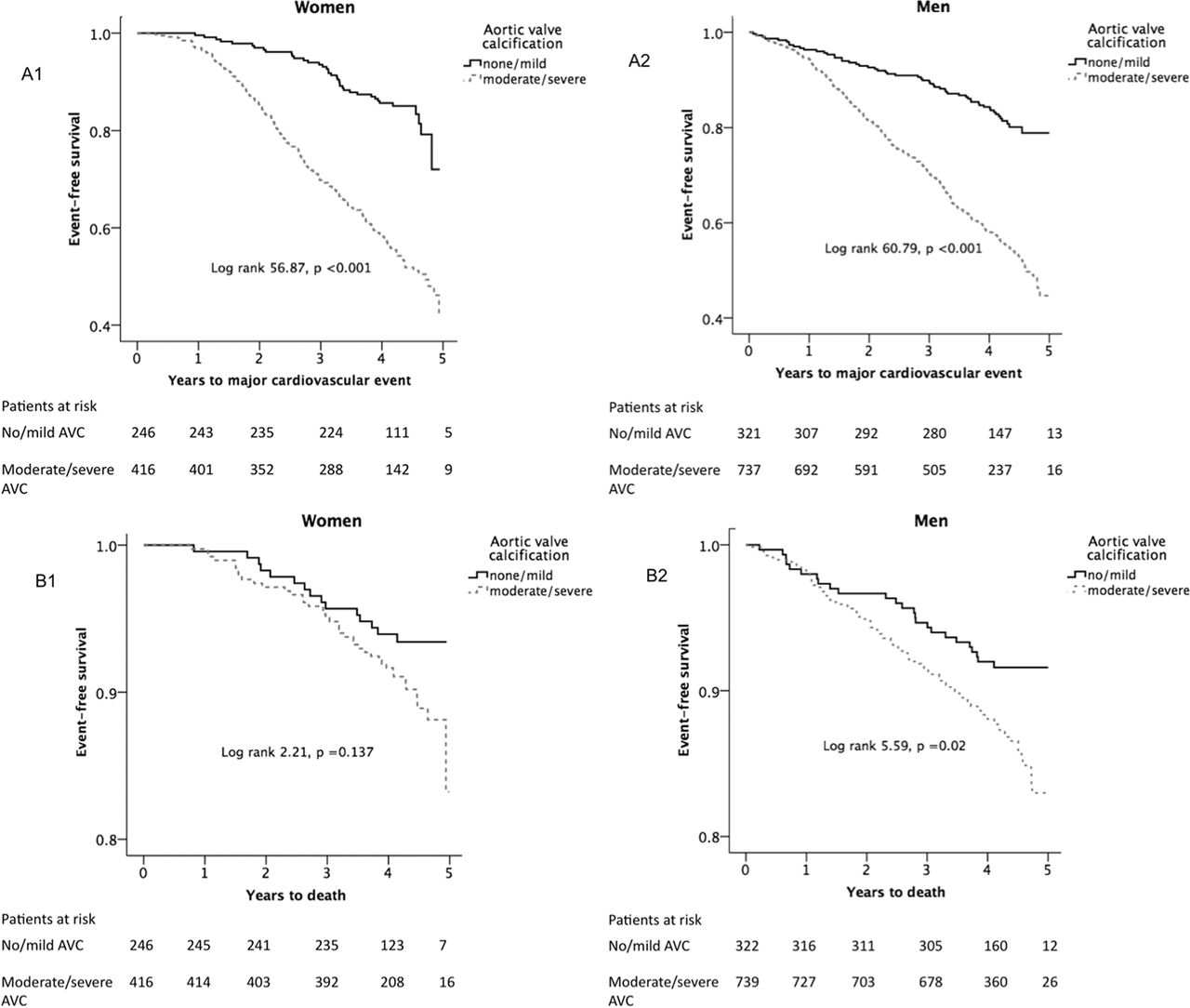
Sex differences also are seen in men and women with calcific aortic valve disease.4 In the 1725 patients with asymptomatic aortic stenosis (AS) enrolled in the Simvastatin Ezetimibe in Aortic Stenosis study (SEAS), aortic valve calcification (AVC) was measured quantitatively by computed tomographic imaging. Interestingly, women had less AVC than men, even though AS was more severe based on haemodynamic criteria. In both men and women, moderate to severe calcification was associated with a higher hazard rate for major cardiovascular events, with a HR of 2.2 (men) to 2.5 (women) compared with no or mild AVC (figure 3).

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier curves reporting survival free of major cardiovascular events (A), and survival (B) in women (left panels) and men (right panels). AVC, aortic valve calcification.
In an editorial commenting on this study, Moura, Rocha-Gonçalves and Gavina5 raise a question: “The findings from this SEAS substudy underline the important pathophysiological differences between women and men and strongly support the development of future research in disease mechanisms specific to each sex and potential individualised interventions. But the question remains: Are we ready to introduce AVC in our recommendation for evaluation and management of patients in AS?” Further studies on this important issue are needed.
The Education in Heart article in this issue focuses on management of acute coronary syndromes (ACS) in women.6 Key points include the differences in presentation of ACS in women and the need for appropriate reperfusion therapy, as well as recognition of sex-related factors in women including pregnancy, menopause and an increased bleeding risk during percutaneous interventions. The authors also emphasise the need for guideline indicated secondary prevention and cardiac rehabilitation in women (table 1).
Sex-related differences in ACS presentation, outcomes and treatment strategy
The Image Challenge question7 in this issue reminds us that women may present with an ACS that is not due to atherosclerotic vascular disease. This coronary angiogram is one that all of us should recognise and know how to treat, particularly in women.
Footnotes
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.