Article Text

Abstract
Objective The excess risk of major coronary events (acute myocardial infarction (AMI) or death from coronary heart disease (CHD)) in individuals with type 1 diabetes (T1D) in relation to glycaemic control and renal complications is not known.
Methods Individuals with T1D in the Swedish National Diabetes Registry after 1 January 1998, without a previous MI (n=33 170) and 1 64 698 controls matched on age, sex and county were followed with respect to non-fatal AMI or death from CHD. Data were censored at death due to any cause until 31 December 2011.
Results During median follow-up of 8.3 and 8.9 years for individuals with T1D and controls, respectively, 1500 (4.5%) and 1925 (1.2%), experienced non-fatal AMI or died from CHD, adjusted HR 4.07 (95% CI 3.79 to 4.36). This excess risk increased with younger age, female sex, worse glycaemic control and severity of renal complications.
The adjusted HR in men with T1D with updated mean haemoglobin A1c (HbA1c) <6.9% (52 mmol/mol) and normoalbuminuria was 1.30 (95% CI 0.90 to 1.88) and in women 3.16 (95% CI 2.14 to 4.65). HRs increased to 10.7 (95% CI 8.0 to 14.3) and 31.8 (95% CI 23.6 to 42.8) in men and women, respectively, with HbA1c >9.7% and renal complications.
Conclusions The excess risk of AMI in T1D is substantially lower with good glycaemic control, absence of renal complications and men compared with women. In women, the excess risk of AMI or CHD death persists even among patients with good glycaemic control and no renal complications.
- diabetes mellitus
- type1
- blood glucose
- myocardial infarction
- coronary disease
- diabetes complications
Statistics from Altmetric.com
Introduction
The onset of type 1 diabetes (T1D) generally occurs in childhood or early adulthood, in contrast to later onset of type 2 diabetes.1 Although several novel treatments have emerged recently, excess risk of mortality associated with T1D persists.2 3
Cardiovascular disease (CVD) is the most common cause of death in persons with T1D,2–4 primarily from coronary heart disease (CHD).5 The Epidemiology of Diabetes Interventions and Complications study showed that intensive glycaemic control reduces the risk of CVD.6 Consequently, current diabetes practice guidelines emphasise optimal glycaemic control.7
Whether the excess risk of AMI persists in Swedish individuals with T1D since these guidelines were implemented is unknown. Using data from the Swedish National Diabetes Registry (NDR), we evaluated risk of AMI and CHD death in persons with T1D in relation to glycaemic control and renal complications.
Methods
This was a nationwide population-based observational cohort study, approved by the ethical committee at the University of Gothenburg, Gothenburg, Sweden.
Study cohort and data sources
The NDR has previously been described in detail.2 8–10 Information is collected by trained nurses and physicians during patient visits at hospital outpatient and primary care clinics nationwide, and reported using electronic records. Clinical data from the NDR were collected and include risk factors, complications within the year of diabetes onset and medications in patients aged >18 years. Verbal and written informed consent was obtained from each patient.
T1D was defined using epidemiological criteria (treatment with insulin and diagnosis aged ≤30 years), which has been validated as accurate in 97% of cases.11 Patients with at least one record in the NDR from 1 January 1998 until 31 December 2011 were included. For each patient,five age, gender and county-matched controls not registered in the NDR were randomly selected from the Swedish Population Register.2 9
Information on comorbidities and cause-specific mortality was retrieved by linking personally identifying information from patients and controls to the Swedish inpatient and cause of death registries. Education and country of birth was retrieved from the Longitudinal Integration database for health insurance and labour market studies.2 Education was categorised as low (compulsory only), intermediate and high (university or similar). Country of birth was categorised as Sweden or other.
The Inpatient Registry includes nationwide coverage of all inpatient admissions from 1987 onwards. International Classification of Disease (ICD) codes were used to define AMI (ICD10 I21, ICD9 410), CHD (ICD10 I20-I25, ICD9 410–414), hospitalisation for heart failure (ICD10 I50, ICD9 428), atrial fibrillation (ICD10 I48, ICD9 427D), valve disease (ICD 10 I05-I09, I34-I36, ICD9 394–396, 424), stroke (ICD10 I61-I64, ICD9 431–434 and 436), cancer diagnoses (ICD10 C00-C97, ICD9 140–208) and renal dialysis and renal transplantation (ICD10 Z49, Z94.0, Z99.2, ICD9 V42A, V45B, V56A, V56W).
Information on prescribed medications was retrieved from the Swedish Prescribed Drug registry, which includes information from July 2005 onwards.12
In the current cohort, patients and controls who had a myocardial infarction (MI) diagnosis before the start of follow-up were excluded. In total, 2.4% (819 of 33 989) of persons with T1D and 3.0% (5127 of 169 825) of controls were excluded due to inconsistent vital status data, leaving 33 170 patients and 1 64 698 controls. Patients and controls were followed from baseline, that is, first NDR record, until non-fatal MI, fatal CHD, 12/31/2011 (date censored) or date of death from non-CHD causes.
Microalbuminuria was defined as two positive tests from three samples taken within 1 year, with an albumin/creatinine ratio of 3–30 mg/mmol (~30–300 mg/g) or U-albumin of 20–200 µg/min (20–300 mg/L), and macroalbuminuria as albumin/creatinine ratio >30 mg/mmol (~>300 mg/g) or U-albumin >200 µg/min (>300 mg/L). Estimated glomerular filtration rate (eGFR) was calculated using the Modification of Diet in Renal Disease equation.13
Procedures
Coronary event rates (AMI or CHD death) were estimated for patients and controls by age (18–34, 35–49, 50–64 and >65 years) and by gender. Age-specific and gender-specific analyses for risk of coronary events were also performed using survival analysis adjusting for the influence of diabetes duration, educational level and coexisting diseases at the start of follow-up.
Survival analysis was used to evaluate the influence of glycaemic control and renal complications on AMI and CHD risk. Patients were categorised by glycaemic control based on updated mean haemoglobin A1c (HbA1c), that is, the mean level of HbA1c until a certain time point.14 HbA1c analyses were performed according to the International Federation of Clinical Chemistry standard measured in mmol/mol and converted to levels according to the National Glycohemoglobin Standardization Program for dual reporting. Renal complications were categorised as normoalbuminuria, microalbuminuria and macroalbuminuria and stage 5 chronic kidney disease (CKD), and further categorised as a separate variable based on eGFR stage 1 (eGFR ≥90 mL/min), stage 2 (eGFR 60–89 mL/min), stage 3 (eGFR 30–59 mL/min), stage 4 (eGFR 15–29 mL/min) and stage 5 CKD (renal dialysis, renal transplantation or eGFR <15 mL/min).
Statistical analysis
Crude rates of coronary events per 1000 patient years, with 95% exact Poisson CIs were calculated. Survival analyses were performed using Cox regression, adjusted for time-updated (the most current value at each event from baseline to end of follow-up) age and gender (model 1), additionally stratified by diabetes duration categories at baseline (aged 0–5, >5–10, >10–15, >15–20, >20–30, >30–40, >40 years) (model 2) and additionally adjusted for education category, birth in Sweden and comorbidities prior to baseline (CHD, atrial fibrillation, heart failure, valve disease, stroke and cancer) (model 3). Model 3 was used to evaluate the association of different time-updated mean HbA1c categories, time-updated albuminuria categories, time-updated eGFR categories as well as time-updated mean HbA1c categories together with albuminuria or eGFR categories in patients with outcomes versus controls. The effect per 10 mmol/mol higher updated mean HbA1c on events was evaluated separately for men and women and adjusted for all variables included in model 3. The influence of other variables was investigated by introducing time-updated mean systolic blood pressure, mean body mass index (BMI), smoking status and use of blood pressure-lowering medications in one model; time-updated mean high-density lipoprotein (HDL) cholesterol, lipid-lowering medication use in a second model; time-updated insulin method (injection or insulin pump) in a third model and time-updated albuminuria categories in a fourth model. Sensitivity analysis was performed to evaluate the effect of HbA1c in the lowest category, ≤52 mmol/mol, among males and females with T1D, and further divided into ≤42, 43–47 and 48–52 mmol/mol categories.
To examine the influence of time (<2005 and ≥2005), Cox regression analysis was used.
The proportional hazards assumption was fulfilled in all instances and was investigated by reviewing the log(-log(survival)) versus log(time) curves.
All tests were two-tailed and conducted at the 0.05 significance level. All analyses were performed using SAS V.9.4 (SAS Institute, Cary, North Carolina, USA).
Results
Baseline characteristics
Baseline characteristics are shown in table 1.
Characteristics of 33 170 persons with T1D and 1 64 698 population-based controls free of prior AMI by categories of HbA1c at first inclusion in the NDR, 1998–2011 (all patients with a prior primary diagnosis of AMI excluded) (ICD9: 410, ICD10: I21)
In total, 33 170 patients and 1 64 698 controls were included. Mean age (35.3 and 35.1 years) and proportion of women (45.3% and 45.1%) was similar. More patients (93.9%) than controls (86.5%) were born in Sweden. Differences in education were comparatively minor.
In patients with T1D, mean HbA1c was 8.2% (65.7 mmol/mol), mean diabetes duration 20.0 years, mean BMI 25.0 kg/ m2, mean blood pressures 126.7/73.6 mm Hg and 86.4% were non-smokers.
Risk of coronary events by age groups and gender in individuals with T1D versus controls
Patients and controls were followed over a median of 8.3 and 8.9 years, respectively. The incidence of AMI and CHD death increased with older age (table 2), with the absolute difference in incidence between patients and controls greatest among older individuals.
AMI or CHD death per 1000 patient years by sex and age categories at baseline with 95% CI estimated by exact Poisson CIs
In all age groups men and women with T1D had almost identical event rates, in contrast to much lower rates in female controls (table 2). Overall, AMI and CHD death in patients was 5.68 cases per 1000 years (95% CI 5.29 to 6.09) for men versus 5.80 (95% CI 5.38 to 6.25) for women. In controls, incidence rates among men and women were 1.90 (95% CI 1.80 to 2.00) and 0.86 (95% CI 0.79 to 0.93) cases per 1000 patient years, respectively.
In Cox regression analysis, the HR for AMI and CHD death adjusted for age and gender was 4.38 (95% CI 4.1 to 4.69) and was slightly attenuated to 4.07 (95% CI 3.79 to 4.36) when additionally adjusted for birth in Sweden, educational level and baseline comorbidities (full model=model 3). HRs for coronary events decreased with older age in both models and were lower for men compared with women in all age groups (figure 1). In the fully adjusted model, the HRs decreased monotonically from 4.72 (95% CI 3.88 to 5.74) among men aged 18–35 years to 2.44 (95% CI 2.09 to 2.87) for men aged 65+ years. The corresponding HRs for women were 18.80 (95% CI 13.26 to 26.54) and 4.38 (95% CI 3.67 to 5.22), respectively.
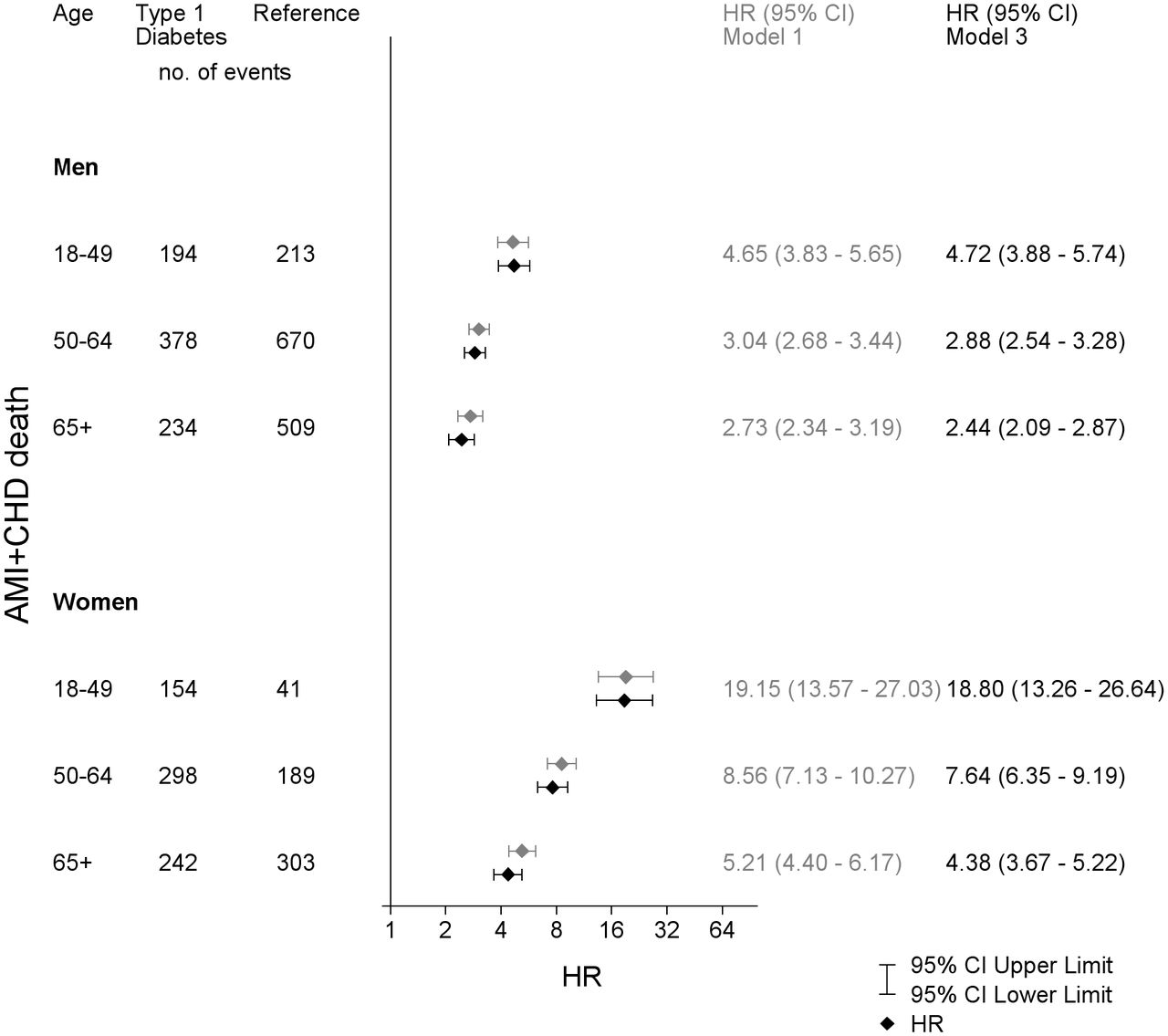
Adjusted HRs for acute myocardial infarction (AMI) or coronary heart disease (CHD) death and 95% CI for patients with type 1 diabetes vs the reference group examined by Cox regression. Model 1 is adjusted for time-updated age and sex, model 3 is adjusted for time-updated age, sex, diabetes duration, born in Sweden, education level, baseline comorbidities (atrial fibrillation, CHD, heart failure, valve disease, stroke and cancer).
Risk of MI in relation to glycaemic control and renal complications
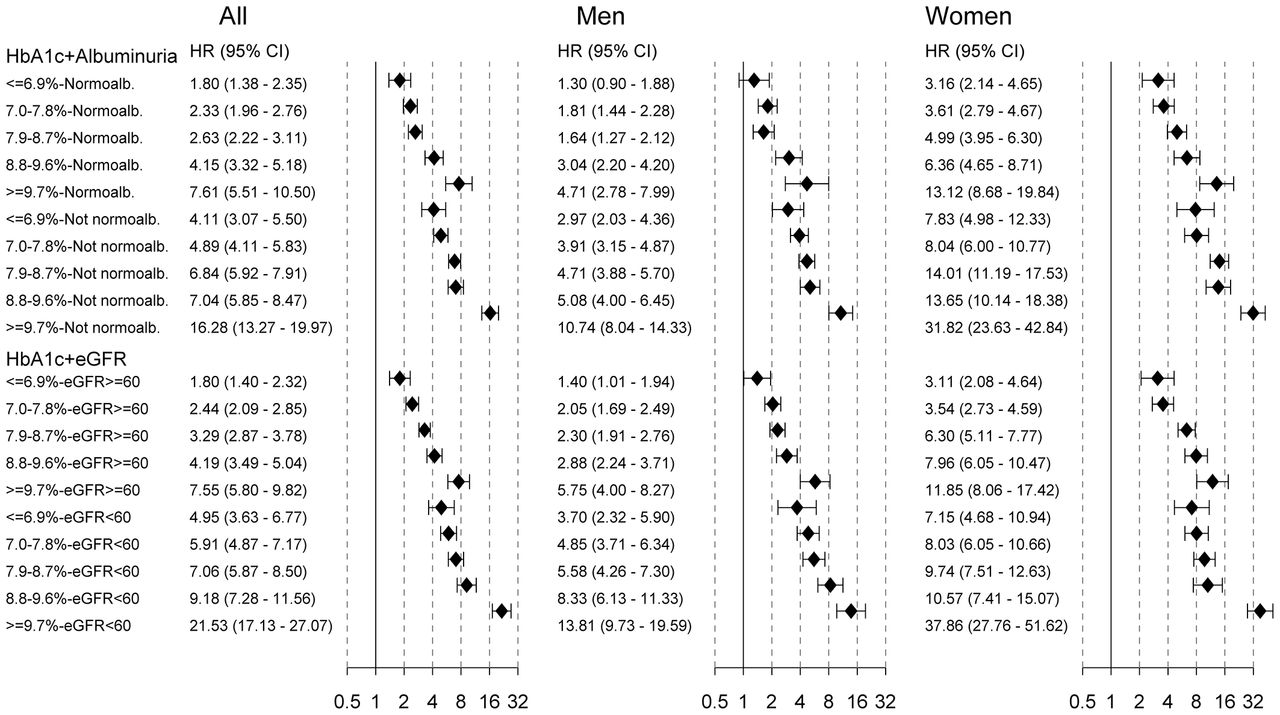
When excess risk for CHD events in patients was evaluated in relation to glycaemic control and renal complications, the relative risks expressed as HRs were consistently higher for women than for men (figure 2).

Adjusted HRs for acute myocardial infarction (AMI) or coronary heart disease (CHD) death and 95% CI for time-updated mean haemoglobin A1c (HbA1c) categories, albuminuria categories and estimated glomerular filtration rate (eGFR) categories vs the reference group examined by Cox regression. p-Values for all comparisons were <0.0001. CKD, chronic kidney disease.
The HRs for men and women with T1D and updated mean HbA1c <6.9% (52 mmol/mol) were 1.86 (1.47–2.34) and 4.37 (3.36–5.68), respectively, compared with controls as a group, increasing with higher HbA1c to 7.46 (95% CI 6.02 to 9.24) and 17.9 (95% CI 14.5 to 22.1), for men and women, respectively, at updated mean HbA1c ≥9.7%. Men and women with normoalbuminuria had HRs for MI and CHD death of 1.86 (95% CI 1.61 to 2.15) and 4.65 (95% CI 3.98 to 5.43), respectively, increasing to 14.5 (95% CI 11.2 to 18.7) and 32.8 (95% CI 24.1 to 44.6) at CKD stage 5, respectively (figure 2). At eGFR ≥90 mL/min, the HRs for men and women were 1.96 (95% CI 1.67 to 2.30) and 4.62 (95% CI 3.66 to 5.84), respectively, increasing with lower eGFR (figure 2). Similar results regarding the effect of eGFR on MI and CHD death were obtained using CKD-EPI (CKD Epidemiology Collaboration) formula (see online supplementary table 1.1, supplementary table 1.2 and supplementary table 1.3), which also includes results from models 1 and 2.
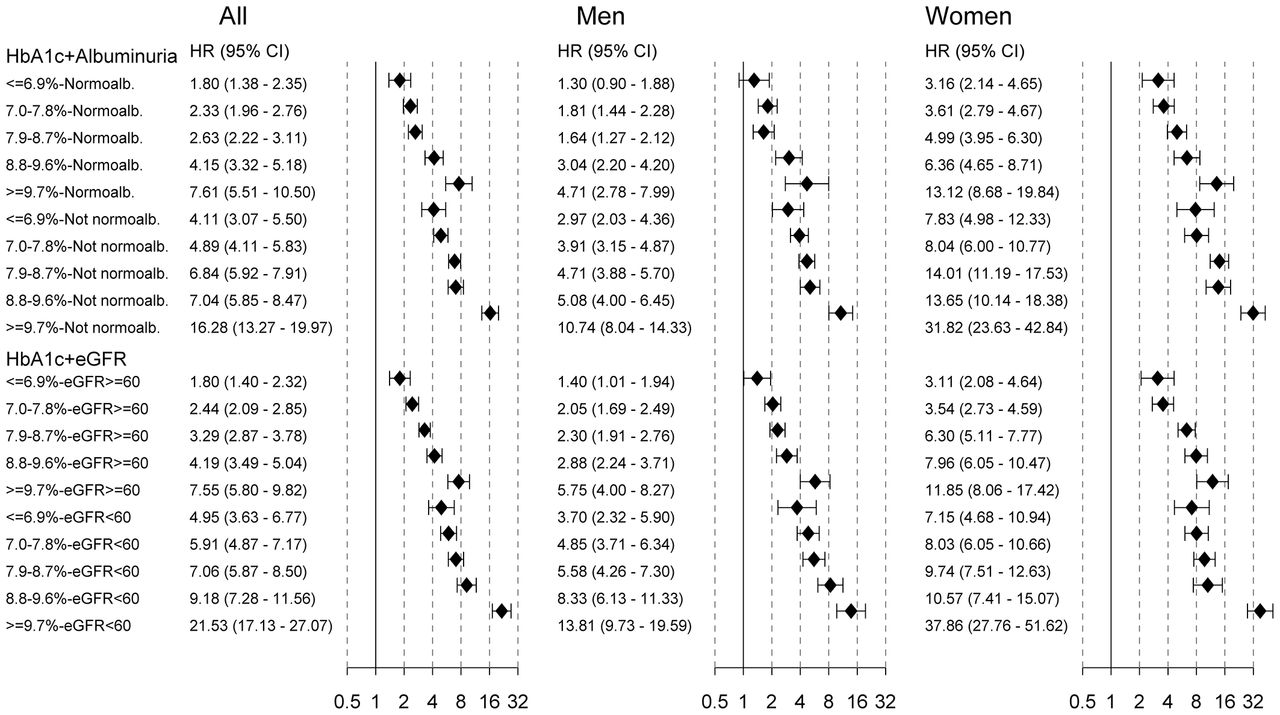
HRs for coronary events for patients with T1D stratified by increasing updated mean HbA1c with coexisting normoalbuminuria and coexisting renal complications are shown in figure 3. Results from models 1 and 2 are available in the online supplementary table 2.1, supplementary table 2.2 and supplementary table 2.3.
{kind=link}
{kind=link}
{kind=link}
Adjusted HRs for acute myocardial infarction (AMI) or coronary heart disease (CHD) death and 95% CIs for time-updated mean haemoglobin A1c (HbA1c) categories together with albuminuria and estimated glomerular filtration rate (eGFR) vs the reference group examined by Cox regression. p Values for all comparisons were <0.0001, except for male ≤6.9% normoalbuminuria where p=0.16, male 7.9%–8.7% normoalbuminuria where p=0.0001 and male ≤6.9% eGFR ≥60 where p=0.049.
HRs for increasing updated mean HbA1c levels for patients with T1D with eGFR ≥60 mL/min versus controls as well as eGFR <60 mL/min are shown in figure 3. HRs were consistently higher for women than men at all levels of HbA1c and renal function.
Risk of MI by 10 mmol/mol HbA1c increase
The relationship between continuous time-updated mean HbA1c (per 1% (10 mmol/mol) increase) and risk of CHD events was investigated among patients with T1D. The HRs for men and women when adjusted for age were 1.33 (95% CI 1.26 to 1.40) and 1.41 (95% CI 1.34 to 1.49), respectively. When adjusted for education, birth in Sweden and comorbidities prior to baseline, the HRs were 1.30 (95% CI 1.23 to 1.38) and 1.41 (95% CI 1.33 to 1.50) per 1% (10 mmol/mol) increase in HbA1c, respectively. There was no statistically significant interaction between sex and continuous HbA1c in these analyses. Clinical characteristics and risk factors in men and women are shown in supplementary table 3. Compared with men, women had higher mean HbA1c during follow-up (p=0.0002), higher baseline smoking rates (p<0.0001), longer diabetes duration (p<0.0001) and lower use of lipid-lowering medication (p<0.0001). Mean systolic blood pressure was lower in women than men (p<0.0001), and HDL cholesterol levels were higher (p<0.0001).
There was no statistically significant difference for time updated mean HbA1c levels ≤42 mmol/mol and 43–47 vs 48–52 mmol/mol for either male or female patients with T1D in the risk of major CHD events (supplementary figure 1).
Risk of MI by calendar year
Later calendar year (≥2005) was associated with decreased excess risk of coronary events compared with controls and in comparison with earlier calendar year (<2005). HRs in patients compared with controls were 3.63 (95% CI 3.33 to 3.95) for calendar years ≥2005 and 4.80 (95% CI 4.26 to 5.42) for calendar years <2005, respectively.
Medications
Among the study population included in the NDR from 2005 onwards and before any coronary event, 25.7% of patients received lipid-lowering medications (Anatomic Therapeutic Chemical (ATC) classification system=C10) after 2005, compared with 4.0% of controls. Renin-Angiotensin-Aldosterone System (RAAS) (ATC=C9) and beta-blockers (ATC=C7) were prescribed to 24.5% vs 5.2% and 11.6% vs 5.9% of patients and controls, respectively. As many as 35.9% of patients received at least one of these medications, compared with 9.8% of controls.
Discussion
The main finding in this nationwide study of persons with T1D in Sweden from 1998 to 2011 is that there was an overall fourfold excess risk of coronary events in patients with T1D compared with matched controls. The excess risk in patients increased with worse glycaemic control and renal dysfunction. The greatest excess risk when using a relative measure (HR) existed in younger individuals, whereas absolute differences were greater in older persons. Regardless of whether a relative or absolute measure was used, the excess risk of MI and CHD death at any age was greater for women with T1D compared with men, explained by a lower incidence of CHD among female than male controls, whereas men and women with T1D had similar rates, implying that women with T1D lose all CHD protective effects of which they normally benefit.
The fact that males have higher incidences of MI than females in the general population has repeatedly been shown, with a 5-year to 10-year delay in first occurrence of MI in women.15 In a systematic review of patients with T1D, Huxley et al reported that women have twice the excess risk of vascular events (both fatal and non-fatal) when compared with men.16 Many theories for this have been proposed, such as differences in insulin resistance, coagulation and cholesterol levels.17 Due to often less clear symptoms in women with CVD, one could speculate about higher rate of undiagnosed cardiovascular events in women in the general population versus patients with diabetes. The mechanisms underlying this difference are unknown and warrant further investigation. Men with diabetes, good glycaemic control and no renal complications had no excess risk of MI compared with male controls, whereas women had at least twice the risk of female controls.
Our findings show that despite advances in treatment, the overall excess risk of coronary events in persons with T1D persists.4 6 17–19 The presence of risk factors such as hypertension or hyperlipidaemia are not as apparent in T1D, compared with T2D, unless in the presence of advanced renal complications, which are often associated with hypertension.20 In T1D, abnormalities in cholesterol and triglyceride plasma levels usually reverse with glycaemic control.21 However, marked hyperglycaemia are features in the majority of persons with T1D. Earlier observational studies of T1D have shown that hyperglycaemia and renal complications are key risk factors for CVD,17 22–28 but these studies did not examine the excess risk in relation to the general population.
Our results show that both optimal glycaemic control and absence of renal complications are associated with markedly lower excess risks of coronary events for persons with T1D than for persons with poor glycaemic control or renal complications, compared with controls. Our results thus support the existing guidelines in T1D, which advocate good glycaemic control to prevent cardiovascular and other complications.
In patients with good glycaemic control, the excess risk for men is approximately double and approximately fourfold for women compared with the general population. However, it is certainly possible that patients with seemingly optimal recent glycaemic control had worse control in the past, which might have contributed to their elevated CHD risk. When evaluating persons with normoalbuminuria as an indicator for reasonably well-controlled glycaemia before the study, males with HbA1c on target had a non-significant 30% excess risk compared with controls. In contrast, the excess risk for women was threefold even in the presence of normoalbuminuria and on target HbA1c. Since normoalbuminuria is a rough marker for earlier good glycaemic control, the current findings must be interpreted with caution as to whether targeting HbA1c from diagnosis onwards will result in similar risk of MI to the general population. It should be noted that women had somewhat higher HbA1c, longer diabetes duration, more were smokers and fewer used lipid-lowering medications. On the other hand, women had lower systolic blood pressure and higher HDL cholesterol levels.
Our results indicate an overall cardioprotective strategy is needed in persons with T1D. Furthermore, in patients with T1D with renal complications such as microalbuminuria or reduced eGFR, and in women (regardless of HbA1c or presence of renal complications), targeting HbA1c may not be enough to reduce the excess risk of MI. In contrast to strategies recommended for the general population, where women are at lower risk, prevention measures in T1D should be the same for women as men.
Although patients with T1D received statin medications, RAAS and beta-blockers more often than the general population, they still had an excess risk. Blood pressure was generally well-controlled, and smoking rates were in line with reports from the general population.29 30 Certainly, specific smoking cessation programmes could be implemented in line with those often used today for patients with previous AMI, since persons with T1D have regular clinical contacts. Continued aggressive treatment with statin medications is likely essential, although clinical trials of lipid-lowering therapies for this patient group are lacking, and the age at which they should be introduced remains unresolved. Finally, non-pharmacological interventions are important, such as physical activity, diet and smoking cessation. Nevertheless, our findings highlight the fact that new, additional cardioprotective strategies are still needed in this patient group, in addition to stricter implementation of measures already known to be effective.
Strengths and limitations of the study
Strengths of the current study include the population-based design, where nearly all patients with T1D in Sweden were included, and use of matched controls. Also the NDR contains comprehensive information on risk factors. Limitations include lacking information on several risk factors of interest at an individual level among controls, such as hypertension and smoking. Also, hypoglycaemia is difficult to record in real life, since the definition is based on glucose level per se (<3.9 mmol/L), which is not always checked in clinical practice on symptoms of hypoglycaemia. Such data were not included in the analyses. Furthermore, patients monitor glucose levels differently, using different frequencies of capillary measurements or flash or continuous glucose monitoring. It cannot be excluded that non-severe AMI may be underdiagnosed to some extent among controls, since persons with diabetes have greater general follow-up rates and closer contact with health providers, thereby possibly detecting more events or resulting in greater referral for additional examinations. Another limitation is that data on the use of cardioprotective medications were available only from 2005. Also, albuminuria was not recorded by exact amount of excreted U-albumin but instead by ‘microalbuminuria’ or ‘macroalbuminuria’, and no sex-specific microalbuminuria cut points were used in the study. Finally, residual confounding cannot be excluded due to the observational nature of this study.
Conclusions
In conclusion, despite treatment advances the excess risk of AMI in patients with T1D remains markedly elevated compared with the general population, although substantially lower in those with good glycaemic control, absence of renal complications and in men. In women, the excess risk of MI remains significantly elevated, even in the presence of good glycaemic control and no renal complications. Aggressive cardioprotective action in persons with T1D is still needed.
Key messages
What is already known on this subject?
Cardiovascular disease is the most common cause of death in persons with type 1 diabetes (T1D), life expectancy in this population is lower. Strategies for optimising glycaemic control have been developed in recent decades.
What might this study add?
The risk of myocardial infarction (MI) is still substantially increased in persons with T1D. The excess risk is greater among women than men. Patients with good glycaemic control and no renal complications have considerably lower risk than others. Excess risk of coronary events was somewhat lower during the second period of follow-up compared with the first period.
How might this impact on clinical practice?
More persons with T1D need to target good glycaemic control to reduce MI to the level of the general population. Future research should continue to focus on other cardiopreventive strategies such as older age, renal complications and history of poor glycaemic control.
Acknowledgments
We thank all of the clinicians who were involved in the care of patients with diabetes for collecting data, and staff at the National Diabetes Registry. The study was financed by grants from Novo Nordisk Foundation and the Swedish state, under the agreement between the Swedish government and county councils for economic support of research and education of doctors (the ALF agreement). This study was also funded by grants from the Swedish Research Council (SIMSAM; grant numbers 2013–5187 and 2013–4236).
References
Footnotes
Contributors All authors (VM-A, AR, A-MS, AP, SG, HW, MK, BH, ML) contributed extensively to the work presented in this paper, discussed the conception and design of the study, interpretation of data and commented on the manuscript at all stages.
Competing interests ML reports receiving honoraria or been consultant for AstraZeneca, Eli Lilly, Medtronic, Novo Nordisk and Pfizer and grant support from AstraZeneca, Dexcom, Novo Nordisk and Pfizer. All other authors declare no conflicts of interest.
Ethics approval Ethical committee at the University of Gothenburg, Gothenburg, Sweden.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data supporting this study are provided as supplementary information accompanying this paper.