Article Text

Statistics from Altmetric.com
Numerous papers address the implementation gap for heart failure management, but most articles include only patients and health assistance in high income countries. In reality, most patients with heart failure live in middle or low income countries where the bottleneck for better care is related to suboptimal health facilities infra-structure, as well as lack of access to basic care and drugs. The study by Carlson and colleagues1 in this issue of Heart sheds light on thisproblem, evaluating the capacity to diagnose and treat heart failure in sub-Saharan Africa. The availability of cardiac diagnostic technologies and select medications for heart failure (β-blockers, ACE inhibitors and furosemide) were evaluated in 197 health facilities in Uganda and 143 in Kenya. Equipment and trained staffing for electrocardiography, ultrasonography and radiography were available generally in less than 50% of studied hospitals. Additionally, only 49% of Kenyan hospitals and 77% of Ugandan hospitals had a medication from each class (selected β-blockers, selected ACE inhibitors and a loop diuretic) and 14%–22% of hospitals reported a major medication stock-out (figure 1). Because heart failure is a major cause of disease burden in sub-Saharan Africa, the authors suggest that “novel low-cost strategies need to be developed and tested in resource-limited settings to reduce these disparities in care”.

Capacity to diagnose and treat heart failure in hospitals in sub-Saharan Africa. Hospitals in Kenya and Uganda had good availability of furosemide and selected β-blockers but poor availability of selected ACE inhibitors. Major medication stock-outs in the preceding quarter (3 months) were fairly common. There was overall poor availability of essential equipment to diagnose heart failure.
In the companion editorial, Rohde and Biolo2 emphasise that, since heart failure is diverse in presentation, management and course across the world, “efforts to reduce these disparities will require a broader understanding of the reality in every region” (figure 2).
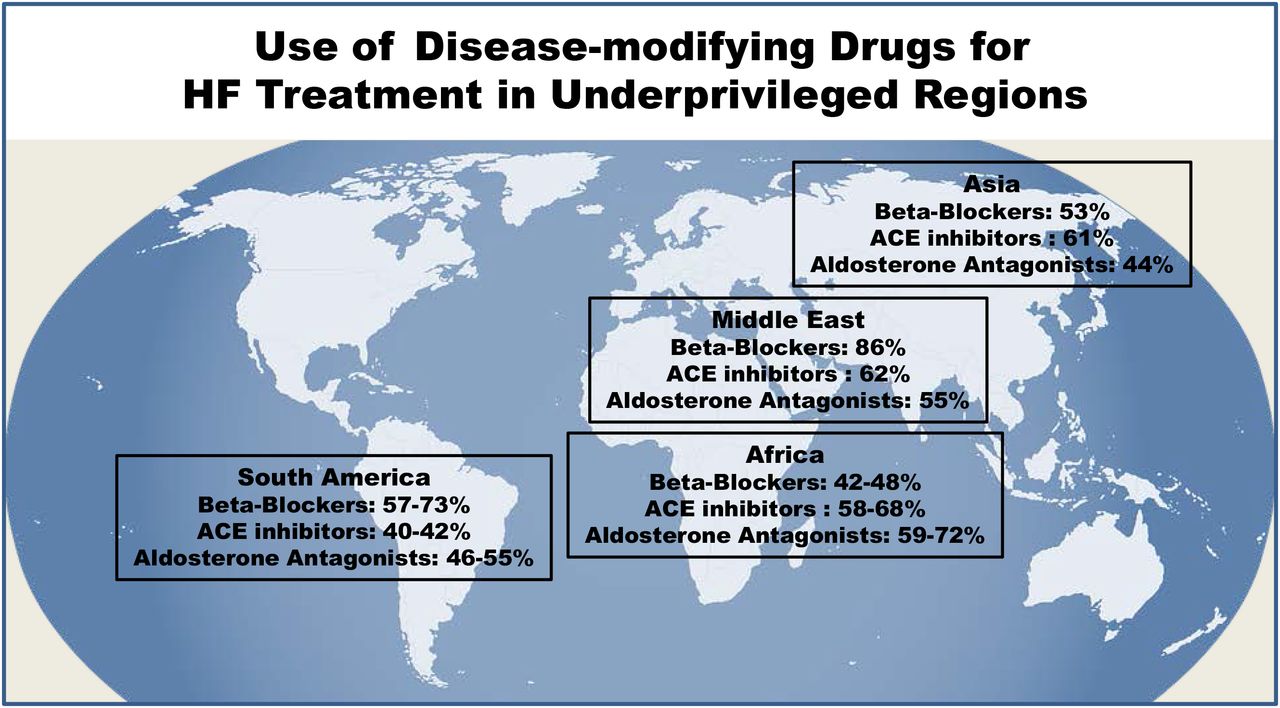
Use of beta-blockers, ACE inhibitors and aldosterone antagonists in South America, Africa, Middle East and Asia according to the INTERnational Congestive Heart Failure Study, the Tanzania Heart Failure Study and Breathe Registry. HF, heart failure.
Geographical disparities in treatment with implanted cardiac electronic devices (CIEDs, including pacemakers and implanted cardiac defibrillators) in sub-Saharan Africa (SSA) are addressed in two point–counterpoint editorials in this issue. Lack of access to pacemaker treatment accounts for over one million deaths per year worldwide, with rate of pacemaker implantation as low as <10 per million population in SSA compared with over 900 per million in European countries. Sani and Mayosi3 note that “In SSA, there are three main barriers for CIED implantation, namely: availability of X-ray facilities with fluoroscopy, lack of clinical expertise and high cost of the devices.” The Pan-African Society of Cardiology (PASCAR) Fellowship in cardiac pacing addresses the second of these issues by training physicians and technologists from underserved SSA countries. They further point out that most CIEDs have residual battery life at the time of the patient’s death and that re-use of these devices would reduce costs for patients in low resource settings. Initial concerns about device infection with re-use of CIEDs have not been substantiated in clinical studies, although there might be a slightly higher rate of device malfunction. However, ethical issues surrounding CIED re-use remain an area of active discussion. Sani and Mayosi3 believe that when patients provide informed consent, “an overemphasis on offering the best therapy (a new pacemaker) may hamper the significant benefits that can be obtained from an otherwise effective treatment (a reused pacemaker), especially when the current alternative for the target population is no treatment at all—the perfect should not be the enemy of the good.”
Tandon, Tate and Kirkpatrick4 discuss the ethical issues in detail and conclude that it is appropriate to perform a randomised controlled trial of reused compared with new pacemakers. However, even if a clinical trial demonstrates safety, “facilities that receive, reprocess and implant used devices should be credentialed to guard against substandard reprocessing and reimplantation practices, a CIED black market and unfair allocation of used devices.” They conclude: “Hundreds of thousands, if not millions, of people around the world suffer from morbid and mortal arrhythmias for which CIEDs are the only durable therapy. Although we must be mindful of the ethical challenges to device reuse, we believe they can be overcome.”
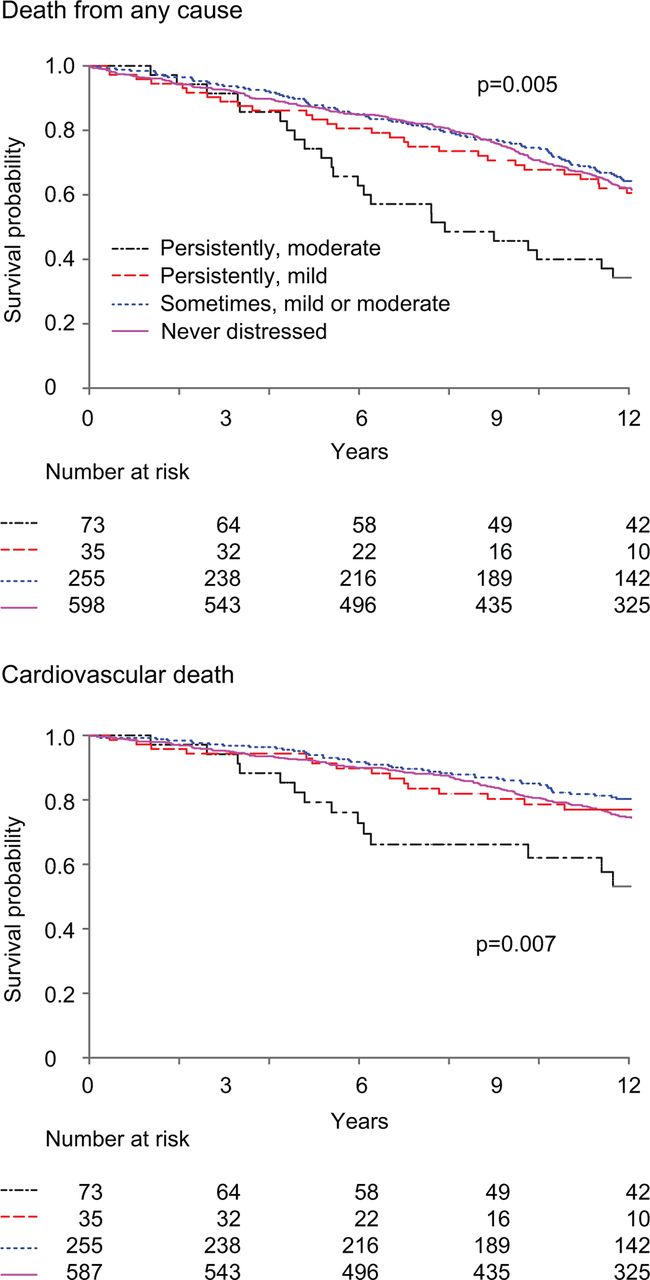
Other papers in this issue include a study in a cohort of 950 patients with ischaemic heart disease showing that moderate or greater persistent psychological distress was associated with a higher risk of cardiovascular death (adjusted HR 3.94, 95% CI 2.05 to 7.56, p<0.001) compared with patients with no distress (figure 3).5
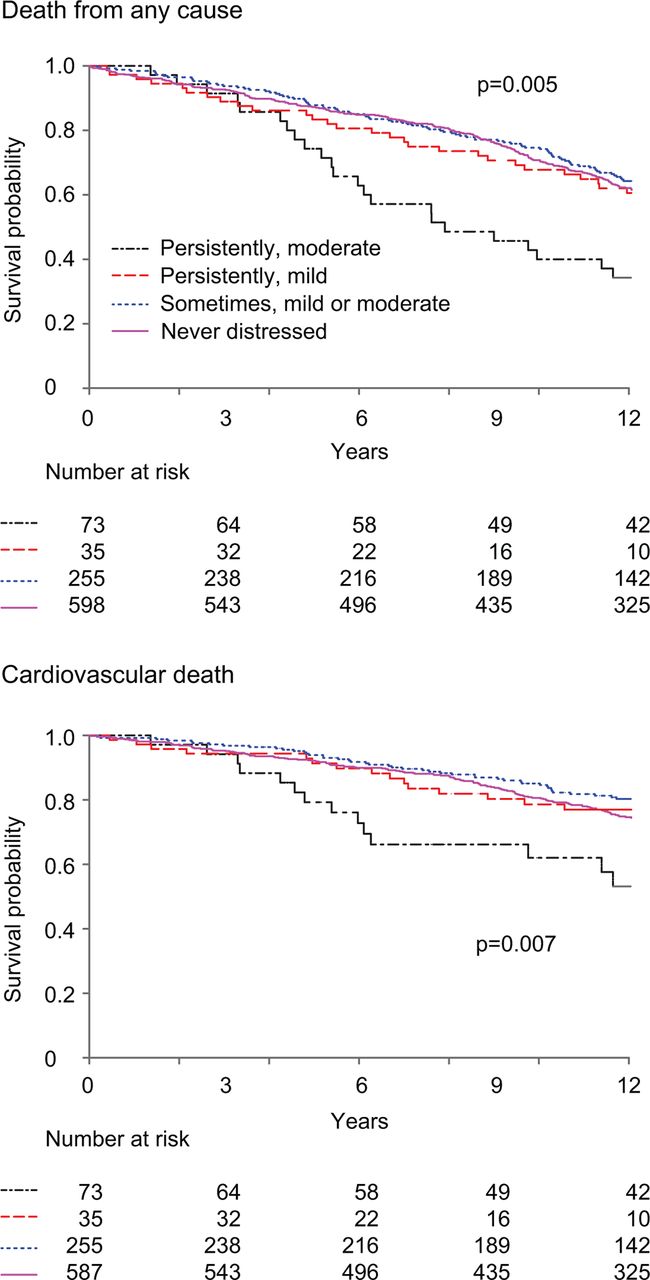
Kaplan-Meier plots of all-cause and cardiovascular mortality after 4 years by no distress, occasional distress and persistent mild and persistent moderate-severe distress during the first 4 years.
In an editorial commenting on these findings, Ndrepepa6 suggests several possible mechanisms for an association between psychological distress and coronary heart disease (CHD) including sympathetic system activation, increased catecholamine levels, elevated inflammation, endothelial dysfunction and a pro-thrombotic state. However, “the question of reverse causality looms largely in studies investigating the association between psychological distress and CHD. The possibility is real that CHD itself is the source of distress and a determinant of poor outcome.” He suggests: “Clinicians should make the screening of psychological distress, a constituent part of the routine assessment of patients with CHD. Strict implementation of secondary prevention measures and referral of distressed subjects to mental health professionals to strengthen their stress-coping aptitude should be included in the strategy of care, principally for subjects with CHD and persistent moderate-to-high distress.”
The Education in Heart article in this issue7 focuses on alternative interventions for refractory angina including pain-focused pragmatic rehabilitation, to help patients self-manage chest pain more effectively, in addition to anti-ischaemic and pain-modulating therapies. In patients with chest pain thought to be due to cardiac ischaemia, a multidisciplinary approach is needed with patient education improve understanding of the pain pathway, correct common misconceptions, helpthe patient set realistic goals, and ensure compliance with medical therapy and secondary prevention. The role of novel drug therapies, percutaneous interventional approaches, biological interventions and alternative non-invasive treatments also are discussed.
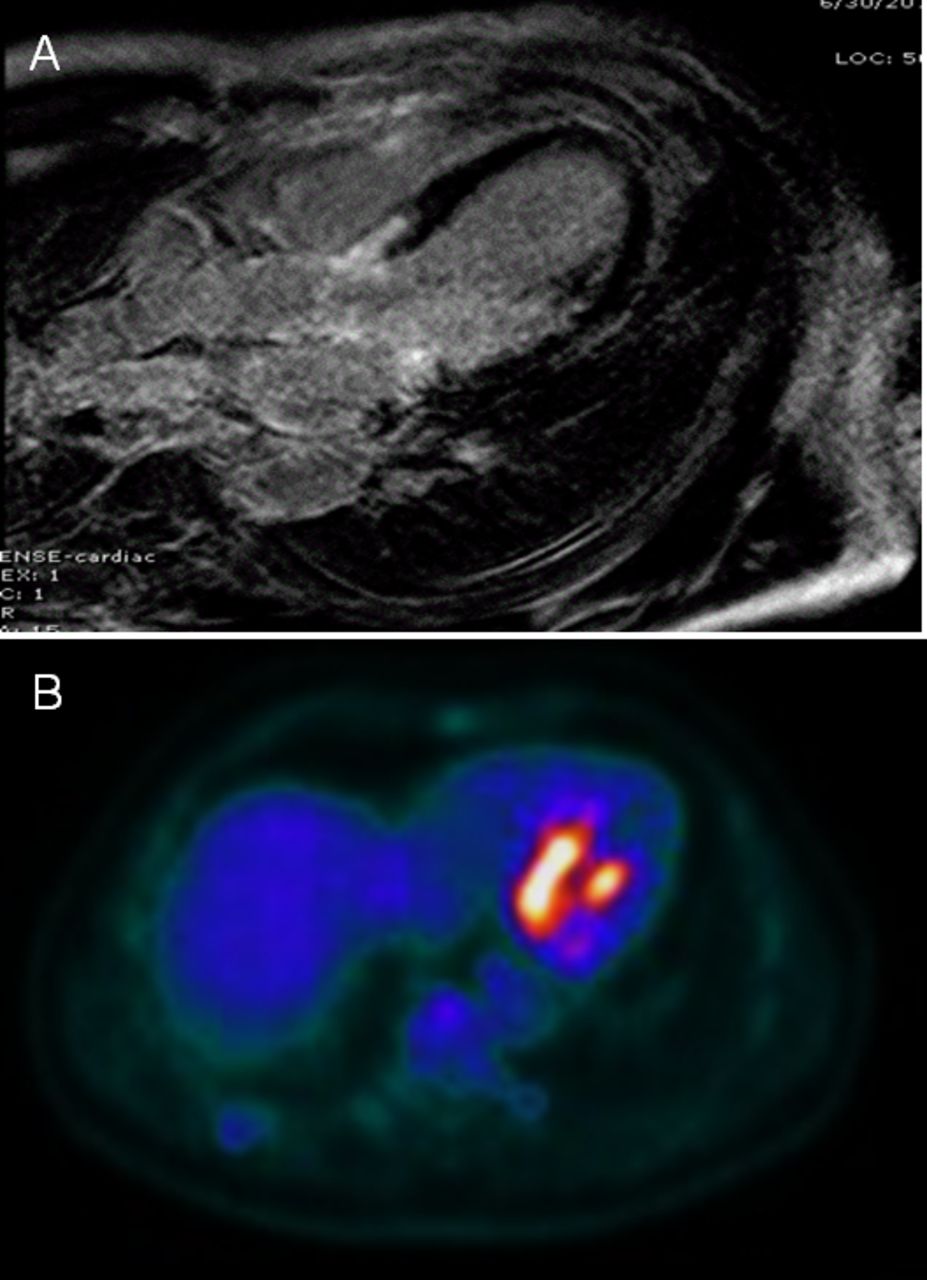
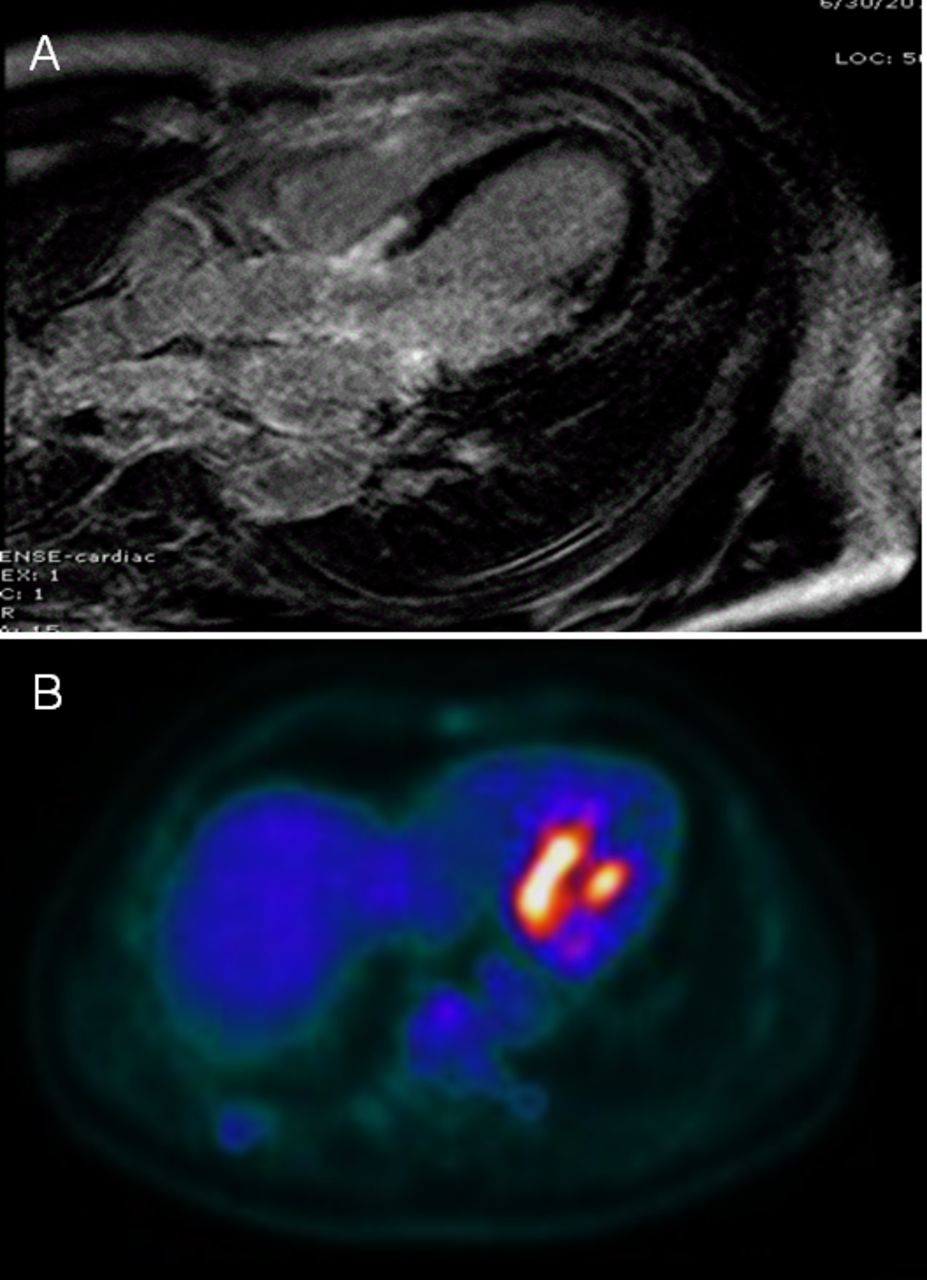
The Image Challenge shows matched cardiac magnetic resonance and positron emission tomography images (figure 4) in a patient with the sudden onset of chest discomfort followed by multiple episodes of ventricular fibrillation. See if you can pick the next most appropriate diagnostic test.8
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cardiac magnetic resonance with a T1-weighted inversion recovery image (A) and 18F-2-fluoro-2-deoxyglucose positron emission tomography (B) in a 54-year-old man with new-onset ventricular fibrillation.
Footnotes
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.