Article Text

Abstract
Objective Atrial fibrillation (AF) is an emerging global epidemic associated with significant morbidity and mortality. Whilst other chronic cardiovascular conditions have demonstrated enhanced patient outcomes from coordinated systems of care, the use of this approach in AF is a comparatively new concept. Recent evidence has suggested that the integrated care approach may be of benefit in the AF population, yet has not been widely implemented in routine clinical practice. We sought to undertake a systematic review and meta-analysis to evaluate the impact of integrated care approaches to care delivery in the AF population on outcomes including mortality, hospitalisations, emergency department visits, cerebrovascular events and patient-reported outcomes.
Methods PubMed, Embase and CINAHL databases were searched until February 2016 to identify papers addressing the impact of integrated care in the AF population. Three studies, with a total study population of 1383, were identified that compared integrated care approaches with usual care in AF populations.
Results Use of this approach was associated with a reduction in all-cause mortality (OR 0.51, 95% CI 0.32 to 0.80, p=0.003) and cardiovascular hospitalisations (OR 0.58, 95% CI 0.44 to 0.77, p=0.0002) but did not significantly impact on AF-related hospitalisations (OR 0.82, 95% CI 0.56 to 1.19, p=0.29) or cerebrovascular events (OR 1.00, 95% CI 0.48 to 2.09, p=1.00).
Conclusions The use of the integrated care approach in AF is associated with reduced cardiovascular hospitalisations and all-cause mortality. Further research is needed to identify optimal settings, methods and components of delivering integrated care to the burgeoning AF population.
- integrated care
- atrial fibrillation
- outcomes
- systematic review
- meta-analysis
Statistics from Altmetric.com
Introduction
Atrial fibrillation (AF) is an emerging global epidemic. In 2010, it was estimated that 33.5 million individuals were living with AF globally, with this figure expected to rise significantly over the coming decades.1 In stark contrast to other chronic cardiovascular conditions which have seen associated declines in mortality, recent data have demonstrated an almost doubling of age-adjusted mortality rates related to AF over the last two decades.1 Furthermore, significant resultant costs are associated with AF, with hospitalisations as the main driver, due to both the condition itself and related complications, including stroke and heart failure.2 Indeed, this rapid increase in hospitalisations has been described as a ‘rising tide’ showing no sign of abate with data suggesting that hospitalisations for AF have now surpassed those related to heart failure.3 4 Both hospitalisation and complications related to AF may be preventable with appropriate guideline adherent care delivery to enhance outcomes in this population. Indeed, current registry data suggest that AF is often suboptimally managed with poor guideline adherence to appropriate anticoagulation for stroke prevention.5 It is clear that a new approach to care delivery is urgently needed to address the burgeoning AF population.
The integrated care approach has its origins in the chronic care model developed by Wagner and colleagues,6 with the recognition that chronic condition management calls for a different approach to more traditional models of care delivery. Central to this model is the patient as the primary focus, with other significant elements, including a multidisciplinary team and community supports, to ensure the patient is actively involved in their management and decisions concerning their care. Enhancing patient outcomes with the use of this model is achieved through redesigning daily practice to ensure care is delivered tailored to the patient’s needs and values, and based on best available evidence.
While a multitude of evidence exists for the use of coordinated systems of care in other chronic cardiovascular conditions, including heart failure7 and acute coronary syndromes,8 there is comparatively less in the AF field. Recently, a number of studies have been undertaken examining the use of integrated care in the AF population,9 10 but until now, a synthesis of the available literature has not been undertaken.
Methodology
This systematic review and meta-analysis was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta- analyses) guidelines.11 The aim of our study was to examine the impact of the integrated care approach in the AF population, compared with usual care, on outcomes including mortality, hospitalisations, emergency department presentations, cerebrovascular outcomes and patient-reported outcomes, including quality of life, anxiety and depression.
Literature search
PubMed, Embase and CINAHL databases were searched from inception to February 2016 with keywords, including ‘atrial fibrillation’, ‘integrated health care’, ‘multidisciplinary’, ‘ambulatory care’, ‘ambulatory monitoring’, ‘outpatient’, ‘interdisciplinary communications’, ‘outcome’, ‘treatment failures’, ‘death’, ‘mortality’, ‘fatal’, ‘hospitalisation’, ‘hospital admissions’, ‘quality of life’ and ‘symptom burden’. See eTable 1 in the supplement for an outline of the full search strategy in PubMed.
Study selection
Inclusion and exclusion criteria
Inclusion criteria were the use of an integrated care approach, focus on holistic and comprehensive AF management, the presence of a control group and a minimum 6-month follow-up period. Randomised and non-randomised studies were eligible for inclusion. Exclusion criteria were studies that focused on one area of AF management (eg, anticoagulation), were not published in English or had less than 50 participants. A previously published description of integrated care was used and was defined as ‘the provision of multidisciplinary care at different stages of the care process in different institutional areas’.12
Data extraction
Two investigators (CG and JH) independently reviewed all relevant articles to identify studies meeting criteria for inclusion. Any discrepancies were discussed and a consensus decision was reached. Data extracted from relevant publications included: first author, years of data collection, year of publication, number of participants, gender balance, mean age, follow-up period, outcomes reported and covariates adjusted for. Risk of bias in each study was assessed using the Cochrane tool.13 See eTable 2 for assessment of risk of bias for included studies. The authors of one study were contacted and provided information concerning all-cause mortality to facilitate report of this as an outcome measure.9
Statistical analysis
The risk estimate for the development of the outcome was extracted from each study. The maximally adjusted model in each study was used. Heterogeneity across studies was assessed using the I2 statistic. The presence of publication bias was visually assessed using funnel plots of effect size against SE. A two-tailed value of p<0.05 was considered statistically significant and all analyses were performed using a random effects model in Review Manager (RevMan) Version 5.3, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Results
The search yielded a total of 1219 articles that were assessed by title and abstract. Of those, 1180 were excluded as they did not meet the inclusion criteria. The remaining 39 articles were retrieved for full-text assessment with three meeting criteria for inclusion in our meta-analysis.9 14 15 The search strategy is depicted in figure 1. Risk of bias was assessed as low in two of the included studies and moderate in one study. The total study population was 1383 and 43% were women. The mean age was 66.9±15.4 years. Characteristics of the three studies included in the meta-analysis are outlined in table 1. Outcomes that were able to be extracted from two or more of the included studies included all-cause mortality, cardiovascular hospitalisations, AF-related hospitalisations and cerebrovascular events. A meta-analysis of results regarding AF-related emergency department (ED) presentations was not performed,as these data were not available in the included studies nor quality of life due to heterogeneity in assessment tools used for this outcome. Similarly, there was a lack of original data on other patient-reported outcomes, including anxiety, depression and symptom burden. Visual assessment of funnel plots did not reveal any evidence of publication bias.

Flow chart of electronic search. AF, atrial fibrillation.
Characteristics of included studies
All-cause mortality
Based on two studies reporting on this outcome, an integrated care approach resulted in a significant 49% reduction in all-cause mortality (OR 0.51, 95% CI 0.32 to 0.80, p=0.003; see figure 2). There was no evidence of significant heterogeneity (I2=0%, p=0.51). The absolute event rate for the intervention group was 3.0 per 100 person-years (95% CI 1.37 to 6.76) compared with 5.7 per 100 person-years in the control arm (95% CI 3.55 to 9.0).

Impact of integrated care on all-cause mortality. [M-H], Mantel-Haenszel method.
Cardiovascular-related hospitalisations
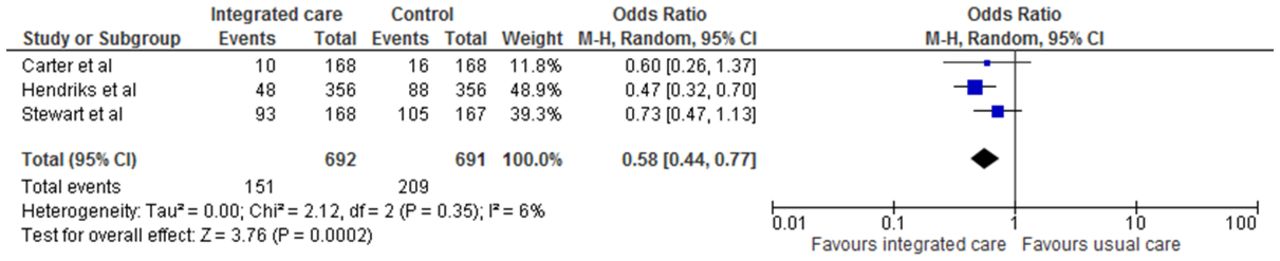
Integrated care was associated with a significant 42% reduction in cardiovascular hospitalisations (OR 0.58, 95% CI 0.44 to 0.77, p=0.0002; see figure 3) based on three studies, without any evidence of significant heterogeneity (I2=6%, 95% CI 0% to 91%, p=0.35). The absolute event rate was 8.0 per 100 person-years in the integrated care arm (95% CI 2.56 to 25.02) compared with 11.87 in the control group (95% CI 4.59 to 30.71). Analysis of this outcome with the exclusion of one study,15 due to a higher risk of bias, did not significantly alter the outcome (OR 0.58, 95% CI 0.38 to 0.89, p=0.01).

Impact of integrated care on cardiovascular hospital admissions. [M-H], Mantel-Haenszel method.
AF-related hospitalisations
The integrated care approach did not have a statistically significant impact on AF-related hospitalisations (OR 0.82, 95% CI 0.56 to 1.19, p=0.29; figure 4) based on two studies reporting on this outcome, without any evidence of significant heterogeneity (I2=0%, p=0.38). An absolute event rate of 5.5 per 100 person-years was demonstrated in the intervention arm (95% CI 1.02 to 29.59) compared with 7.0 per 100 person-years in the control group (95% CI 1.87 to 26.23).

Impact of integrated care on atrial fibrillation-related hospital admissions. [M-H], Mantel-Haenszel method.
Cerebrovascular events
Similarly, there was no evidence of any benefit of an integrated care approach on cerebrovascular events based on three studies reporting on this outcome (OR 1.00, 95% CI 0.48 to 2.09, p=1.00; figure 5). There was no evidence of significant heterogeneity (I2=0%, 95% CI 0% to 73%, p=0.68). There were comparable absolute event rates in both arms of the study at 1.1 per 100 person-years in both groups (95% CI 0.50 to 2.44 for the intervention group and 95% CI 0.66 to 1.82 for the control group). Exclusion of one study from this analysis,15 due to a higher risk of bias, did not significantly alter this result (OR 1.00, 95% CI 0.42 to 2.38, p=1.00).
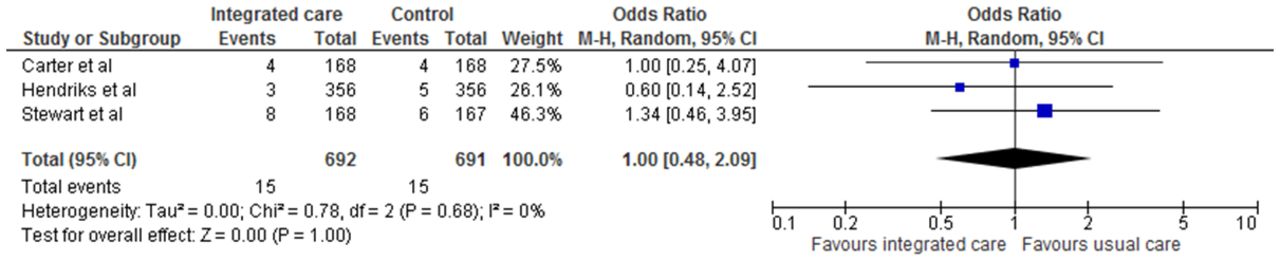
Impact of the integrated care approach on cerebrovascular events. [M-H], Mantel-Haenszel method.
Patient-reported outcomes
A meta-analysis of results related to quality of life or anxiety and depression was not possible due to heterogeneity of assessment tools used across studies. Two studies reporting on quality of life outcomes did not report any statistically significant between- group differences at final follow-up and, similarly, no impact of an integrated care approach on either anxiety and/or depression was demonstrated.14 16 None of the included studies reported on effect of the intervention on symptom burden.
Number needed to treat (NNT)
Statistically significant outcomes were further analysed to determine a number needed to treat (NNT) compared with published data for heart failure clinics.17 For all-cause mortality, a NNT of 19 in an AF programme was demonstrated to prevent one death, compared with 17 in heart failure clinics. With respect to hospitalisations, the NNT was 18 in anAF care programme to prevent one cardiovascular-related hospitalisation, compared with 11 in a heart failure clinic to prevent one heart failure-related hospitalisation.
Discussion
Major findings
This meta-analysis of studies evaluating the role of an integrated care approach in AF demonstrates that integrated care is associated with:
enhanced patient outcomes, including reduction in all-cause mortality and cardiovascular hospitalisations;
no significant impact of an integrated care approach on AF-related hospitalisations and cerebrovascular events;
insufficient original data to report on a synthesis of data related to patient-reported outcomes;
a highly efficacious NNT which compares favourably with other approaches, including coordinated heart failure care programmes, for outcomes including all-cause mortality and hospitalisations.
These findings have significant implications regarding care delivery in the AF population and support the use of integrated care as an effective and efficacious intervention. However, many questions remain unanswered and further research is required to address the way in which delivery of this approach is optimally implemented.
Studies on integrated care of AF
Whilst each study used an integrated care approach, there are significant differences in populations recruited and methodology employed for care delivery within this approach. The first study by Hendriks and colleagues was a single-centre study undertaken in the Netherlands.9 This study recruited participants who had been referred to the outpatient clinic for management of AF and randomised half of them to a nurse-led, cardiologist supervised clinic. The programme incorporated protocoled diagnostic testing, patient education and recommendations for AF management based on current guidelines at the time. The study also employed a software decision support system to facilitate guideline adherence, guide treatment recommendations and support decision making. After a mean follow-up of 22 months, there was a significant 35% reduction in the composite endpoint of cardiovascular mortality and hospitalisations (HR 0.65; 95% CI 0.45 to 0.93; p=0.017).9
The Standard versus Atrial Fibrillation-specific strategy (SAFETY) study was a multicentre Australian-based study in which participants who were admitted to hospital primarily due to AF were eligible for inclusion in the study.10 The intervention was diverse and included a home visit undertaken by a specialised cardiac nurse 7–14 days postdischarge, an education package, referral to other healthcare professionals, including physician referral for those requiring urgent review at the home visit, and recommendations to the medical team concerning optimal AF treatment. After a mean follow-up of two and a half years, there was proportionately more event-free days in the intervention group (defined as days alive and out of hospital) but no significant difference in the coprimary composite outcome of all-cause mortality and hospitalisations (HR 0.97, 95% CI 0.76 to 1.23; p=0.851).
The final study was a ‘before and after’ study undertaken in Canada with eligible participants having presented to the emergency department primarily due to symptoms arising from AF.15 In the intervention phase, participants received a brief educational telephone call by a cardiac nurse following discharge, were invited to attend a group education session and undertook one clinic visit in a nurse-led, cardiologist supervised clinic. In propensity matched groups, the primary composite endpoint of all-cause death, cardiovascular hospitalisations and AF-related ED visits was statistically significant (OR 0.71; 95% CI 0.59 to 1.0; p=0.049).
Despite differences employed in each study, we did not find any evidence of statistically significant heterogeneity in any of our outcomes, strengthening the conclusions drawn from our results. However, it is of interest to further explore each of these studies to explore clinical applicability and direct areas for future research. Although none of the studies were appropriately powered for all-cause mortality as an outcome measure, it is encouraging that coordinating care through an integrated approach had a clear and consistent effect in the two studies reporting on this. Similarly, the positive impact on cardiovascular hospitalisations is also consistent, although reasons for the impact on this outcome but not AF hospitalisations are of interest. First, how much of the reduction in cardiovascular-related hospitalisation is due to enhanced clinical surveillance and improvements in cardiovascular risk factor status is not well defined. Two of the three studies did not report on changes in cardiovascular risk factor status, while the SAFETY study did not find any significant difference in any cardiovascular risk factor measures between groups at final follow-up. Recently, the role of intense management of cardiovascular risk factors in the AF population has gained significant momentum with the recognition that this approach is associated with reduced symptom burden and greater AF ablation success.18–20 It is also possible that participants having access to specialist care when required could have prevented cardiovascular-related hospital admissions. The lack of impact on AF-related hospitalisations is somewhat surprising but perhaps reflects a generally sicker population with comorbidities accounting for the need for hospitalisation. It is also possible that this reflects a type 2 error due to a small sample size and a significant impact may be observed in a larger population. Similarly, cerebrovascular events were not significantly reduced with the use of this approach. This perhaps belies the complex issue of anticoagulation, with numerous issues, including the informed decision of the patient, to take into consideration. It may also reflect the need for enhanced surveillance and management of cardiovascular risk factors with increased recognition that both AF and stroke share common risk factors and this may play a significant part in the pathogenesis of cerebrovascular ischaemic events in AF. Encouragingly, recent data have suggested a significant increase in appropriate use of anticoagulation based on CHA2DS2-VASc score, with the clinical adoption of novel oral anticoagulant therapy,21 which was not in widespread use at the time two of the three studies were undertaken.
Two of the studies reported on appropriate prescription of anticoagulation based on CHADS2/CHA2DS2-VASc (C-Conjestive heart failure, H- Hypertension, A-Age 75 years and older, D-Diabetes mellitus, S-prior Stroke /TIA or thromboembolism, V-Vascular disease, A-Age 65–74 years, Sc - Sex category (i.e, female gender)) score9 10 with a significantly greater rate in the Hendriks study warranting further exploration. While it is clear from the baseline demographics that the SAFETY study had a generally sicker and comorbid population, the method by which anticoagulation was addressed may also be relevant. As a clinic-based study, Hendriks and colleagues were able to initiate anticoagulation and discuss any relevant issues at subsequent visits, while the SAFETY study made recommendations to treating clinicians without being able to start appropriate antithrombotic therapy if it was indicated. This should be a consideration for future studies as it is a phenomenon other studies have also found with appropriate therapy often not initiated unless it is undertaken by the specialist clinic.22 The importance of both integrated care in AF and cardiovascular risk factor management in this population has recently been enhanced as recent guidelines have recommended these approaches as part of standard care delivery.23
There were insufficient original data to undertake a meta-analysis on patient-reported outcomes due to either lack of report on these outcomes or heterogeneity in assessment toolsused. This is a point worthy of consideration in the design of future studies in this field. The use of standardised clinical and patient-reported outcome measures in AF, such as those recommended by the International Consortium for Health Outcomes Measurement (ICHOM) for coronary heart disease24 and heart failure,25 would be of significant benefit in both future research in this field and in design of optimal care delivery systems for clinical application and evaluation.
Strengths and limitations
The results of this meta-analysis point to integrated care as a highly effective method of care delivery, which is further strengthened by examining outcomes in studies which have a control group undertaking usual care, to provide a high level of evidence on the effectiveness of the integrated care approach. However, several limitations need to be considered with regard to the current study. First, while it is clear that the integrated care approach is associated with enhanced patient outcomes, it is difficult to know which components of this approach, and to which AF subpopulation, it would be of most benefit. Second, the setting and personnel required varied between studies and may need to be individualised with the recognition of AF as a heterogeneous condition with patients often having complex and competing needs, making appropriate recommendations in this area difficult. A schematic of how the integrated care approach may be applied in the AF population has previously been described and is outlined in figure 6.26 This highlights the importance of the multidisciplinary team approach with the patient at the core, and decision support systems to facilitate delivery of best practice, guideline adherent care. The possibility that an impact of the integrated care approach on both AF-related hospitalisations and cerebrovascular events may be observed in a larger sample size also needs to be taken into consideration due to a type 2 error in the current study. Finally, the need for clearly described methodology to allow for replication of studies is difficult due to the nature of such interventions, but would be of benefit to the clinical and research community in determining how best to apply this approach.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Suggested schematic for application of the integrated care approach in atrial fibrillation (AF) (modified and reproduced from Lau et al)26.
Conclusions
This meta-analysis of current evidence demonstrates integrated care as a highly effective intervention when applied to the AF population with associated reductions in all-cause mortality and cardiovascular-related hospitalisations. The integrated care approach, now recommended by international AF guidelines, has a crucial role in improving outcomes in this rapidly increasing population and should be widely implemented in the clinical setting. However, further work is needed to refine the optimal settings, methods and components of care delivery in such approaches, with strong consideration given to standardised clinical and patient-reported outcomes in the AF sphere.
Key messages
What is already known on this subject?
Coordinated systems of care have demonstrated improved patient outcomes in other chronic cardiovascular conditions, including heart failure and acute coronary syndrome. Recognition of atrial fibrillation (AF) as a chronic cardiovascular condition has led to the development of care delivery programmes with a view towards improving outcomes in this population. Integrated care has been proposed as an alternative model of care delivery with early data suggesting that this approach is beneficial in the AF population.
What might this study add?
This study demonstrates that the use of an integrated model of care delivery in AF is associated with enhanced patient outcomes, including reduced all-cause mortality and cardiovascular hospitalisations.
How might this impact on clinical practice?
Given the significant global burden of AF, integrated care models should be widely implemented and evaluated in clinical practice with further research needed to identify optimal components of care delivery. Consideration should be given to standardised health and patient-reported outcomes to facilitate clinical application and evaluation.
References
Footnotes
Contributors CG, JH and PS had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: CG, JH and PS. Acquisition of data: CG and JH. Analysis and interpretation of data: CG, JH, AE, DL and PS. Drafting of the manuscript: CG, JH and PS. Critical revision of the manuscript for important intellectual content: CG, JH, AE, CXW, GR, MM, RM, DL and PS. Statistical analysis: CG and AE. Administrative, technical or material support: CG, JH, AE, CXW, GR, MM and RM. Study supervision: JH, CXW, DL and PS.
Competing interests None declared.
Patient consent This manuscript contains a systematic review. Consent and ethics procedures have been undertaken in the original studies.
Provenance and peer review Not commissioned; externally peer reviewed.