Article Text

Statistics from Altmetric.com
Although many patients requiring long term anti-thrombotic therapy now can be treated with direct oral anticoagulants (DOACs), vitamin K antagonists, such as warfarin, remain the only treatment option in patients with mechanical heart valves (MHVs). In the future, we can expect that fewer patients will receive (MHVs), given that surgical repair often is possible in patients with mitral valve disease and a bioprosthetic valve is appropriate in older adults with aortic valve disease. However, there still is a group of younger patients in whom the benefits of long term valve durability with a MHV outweigh the risks of warfarin anticoagulation.
Management of warfarin therapy can be challenging given the need for frequent dosage adjustment to maintain adequate anticoagulation, with the international normalized ratio (INR) varying with changes in diet, physical activity, concurrent medications, patient compliance and other factors. Grzymala-Lubanski and colleagues (see page 198) examined data from a cohort of 4687 patients with MHVs entered into a Swedish National Quality Registry over a 5-year period to examine the risk of bleeding in relation to time in therapeutic range (TTR) and variability in the INR level. Overall, the rate of thrombotic events was 2.41 per 100 treatment-years. Major bleeding occurred in 3.15 per 100 treatment-years; the rate of intracranial hemorrhage, the most devastating bleeding complication in young adults, was 0.47 per 100 treatment-years. A lower TTR (≤70%) was associated with a higher risk of bleeding (HR=2.43, 95% CI 2.02 to 2.89, p<0.001) with no significant difference in thrombosis rates (table 1). A greater degree of INR variability was associated with higher rate of all complications, including both bleeding and thrombosis. Higher intensity anticoagulation did not reduce the risk of thrombosis but was associated with increased bleeding risk with an adjusted hazard ratio of 2.92 (CI 2.39 to 3.47) comparing an actual INR of 2.8 to 3.2 versus 2.2 to 2.7.
Rate of complications per 100 treatment years with 95% CI, according to MHV position, intended INR target, or warfarin treatment quality measured as TTR or INR variability, using TTR 70% or the mean INR variability of 0.40 as cut-off
In the accompanying editorial, Iung (see page 179) comments that MHVs still account for about 20% of implanted valves in Europe, highlighting the need for better quality anticoagulation in these patients. The data in the study from Sweden reflect real-world experience in a system that uses a computerised dosing system allowing for good INR stability, and convincingly demonstrate the combined effects of TTR and INR variability on clinical outcomes. Iung suggests that “The combined use of TTR and INR variability therefore appears as an attractive surrogate endpoint for developing strategies aimed at optimising INR stability.” Such strategies might include management by dedicated anticoagulation clinics, use of home INR monitoring, and specifying a narrow INR target range. “Current evidence supports the use of target INRs from current guidelines, which are largely consistent between European and American guidelines. Nevertheless, there is a rationale to plan well-designed and adequately powered randomised trials to further refine the definition of optimal target INR in patients with mechanical prostheses.”
Also in this issue, Allan and colleagues (see page 210) looked at the net clinical benefit of warfarin therapy for stroke prevention in over 70 thousand patients with atrial fibrillation (AF) comparing those in whom the initial diagnosis of AF was made by primary (42%) versus secondary (58%) care in England over a 12-year period. Net clinical benefit was defined as the number of ischemic strokes avoided per 100 patient-years of warfarin therapy. The authors found that the CHA2DS2-VASc score accurately stratified ischemic stroke risk in patients initially diagnosed in either primary or secondary care. However, patients initially diagnosed in primary care settings had lower risk scores and fewer strokes than those diagnosed by secondary care providers; the ischemic stroke rate was 2.3 (2.2 to 2.4) per 100 patient-years in primary care versus 4.3 (4.2 to 4.4) per 100 patient-years in secondary care. A CHA2DS2-VASc score of 2 or greater was associated with a positive net clinical benefit in men compared to a score of 3 or greater in women (figure 1). The authors raise the concern that their data did not show benefit of warfarin anticoagulation in those with a score of 1, although only about one quarter of all patients had a CHA2DS2-VASc score of 0, 1 or 2 in this population.
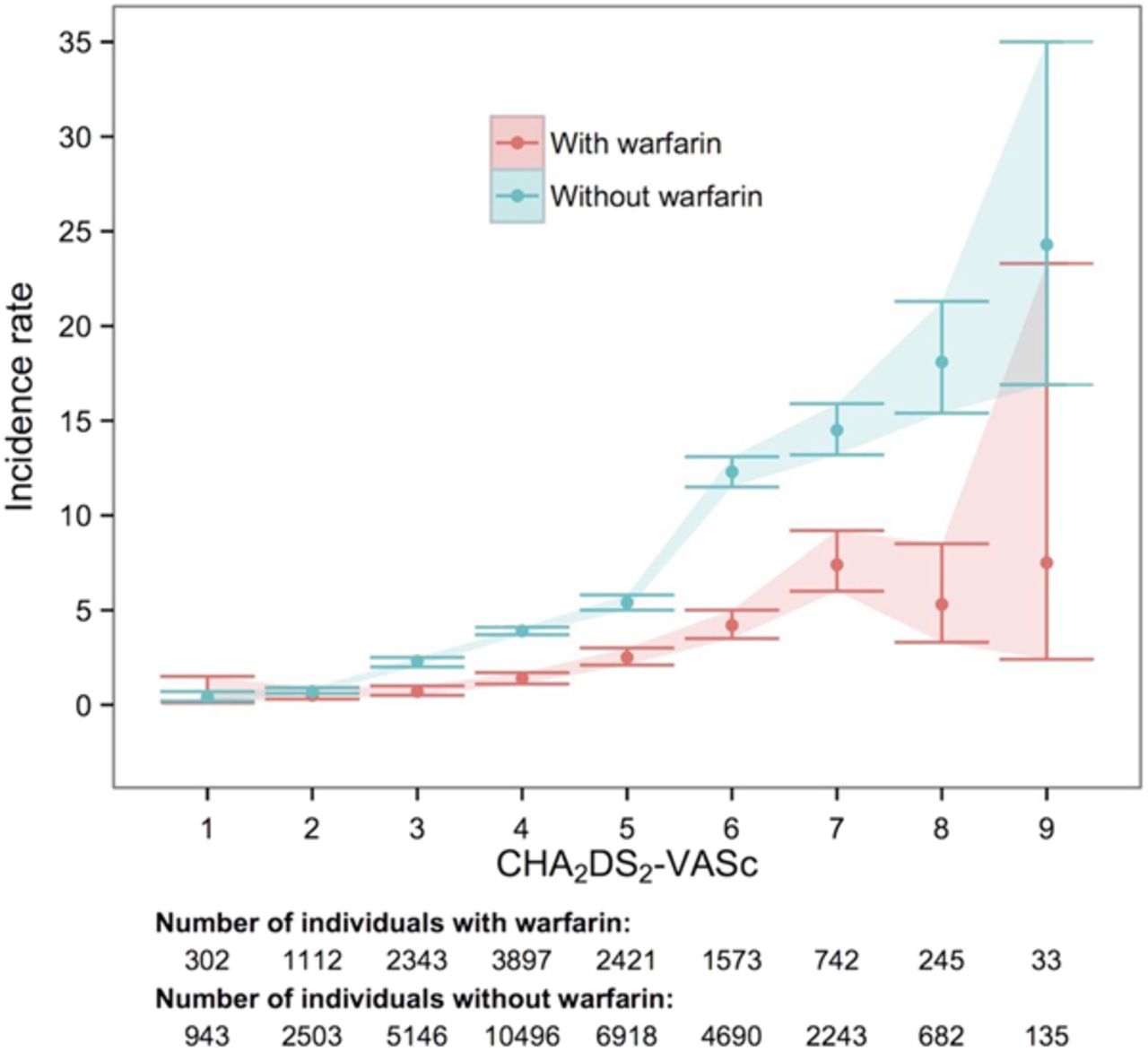
Incidence rates (95% CIs) per 100 person-years of ischaemic stroke in women by CHA2DS2-VASC scores, and use of warfarin. Individuals could contribute follow-up time to periods with and without warfarin.
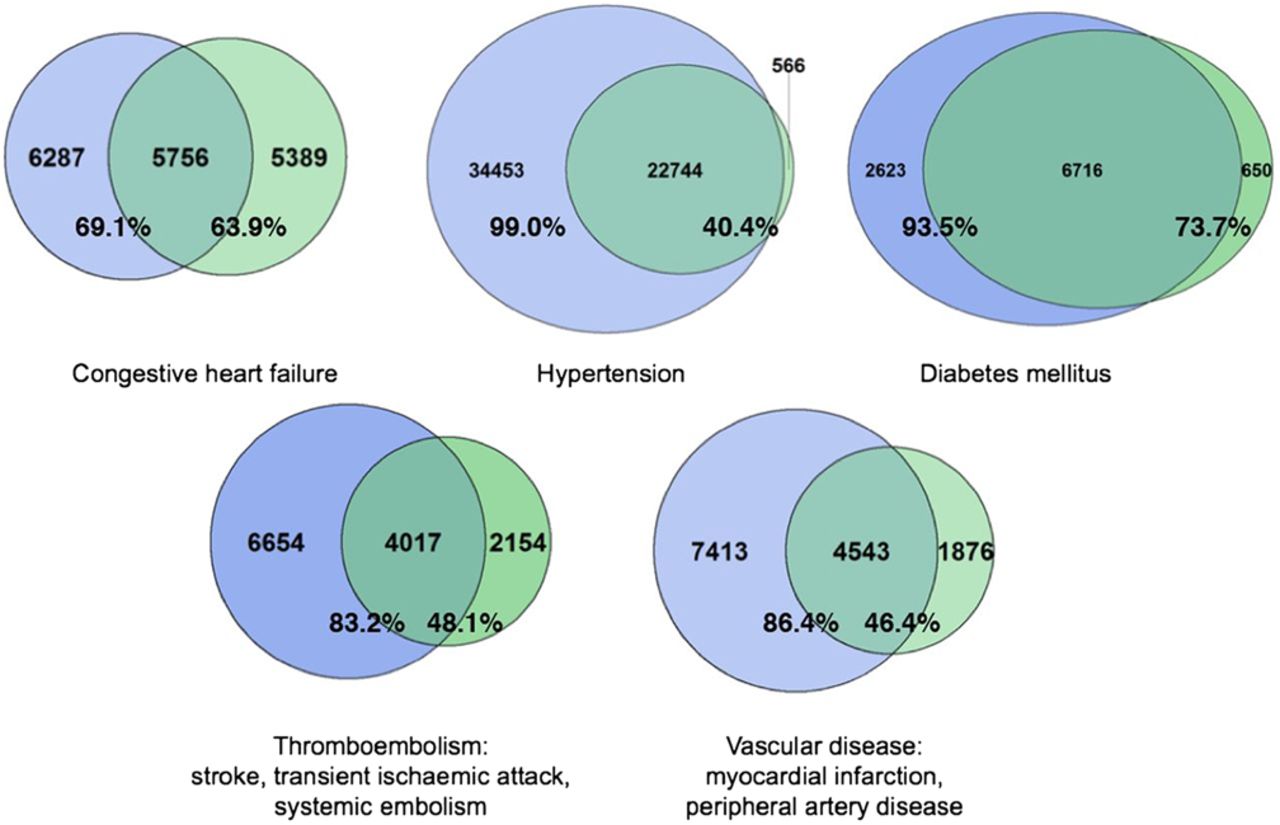
Heidbuchel points out important caveats in an editorial accompanying this paper (see page 181). Complete and accurate capture or risk factors is needed for classification of stroke risk and many patient records were still incomplete even when primary and secondary care information were combined (figure 2). He suggests “Primary care physicians and hospitals should implement systematic and robust classification schemes for patients with AF to guide management, especially since CHA2DS2-VASc is confirmed to be a universally valid stroke risk scheme.” Other considerations include: (1) Warfarin therapy was provided in less than ½ the population and adequacy of warfarin anticoagulation, for example time in therapeutic range, was not included in the analysis. (2) The current study only considered ischemic stroke, not other ischemic events such as transient ischemic attacks, pulmonary embolus or myocardial infarction. (3) Among bleeding events, only hemorrhagic stroke was included in the analysis, and (4) The net clinical benefit of DOACs was not evaluated in this study even though these newer medications have replaced warfarin for prevention of stroke in many AF patients.

Venn diagrams comparing numbers of CHA2DS2-VASc risk factors captured in primary care (blue), secondary care (green) and in both sources linked (combined). The percentages indicate the completeness of recording different risk factors in primary and secondary care records. Venn circles are scaled according to the proportion of individuals.
Assessment of the severity of mitral regurgitation (MR) by Doppler echocardiography relies on integration of several parameter, including quantitative measures of regurgitant severity. One of the qualitative measures used in many centers is the density of the continuous wave (CW) Doppler MR flow curve relative to the antegrade flow signal. El-Haddad and colleagues (see page 190) show that measurement of the average pixel intensity (API) in the CW Doppler MR signal provides a quantitative measure that has low intra-and inter-observer measurement variability and compares well with other echocardiographic indices of MR severity (figure 3).

{kind=link}
{kind=link}
{kind=link}
Continuous wave signal intensity analysis in mitral regurgitation: Representative CW envelopes in patients with different grades of MR. The coloured CW envelopes are converted to a greyscale (0–255 au) envelope and the area of interest is traced manually. The PI histograms display the distribution of the pixels according to their intensity value. Besides each histogram, several statistical parameters are given. API, average pixel intensity; au, arbitrary unit; CW, continuous wave; MR, mitral regurgitation; PI, pixel intensity.
Hung and Levine (see page 177) suggest that this proposed new method “is a step towards the holy grail of MR quantification: a simple, reproducible and automated technique to quantify MR flow.” However, “MR flow quantification is a complex beast and it is naïve to think (nor intended by the authors) that the method described by El-Haddad et al is a comprehensive and definitive solution to this problem. Although a step in the right direction, there are important factors that need to be taken into account.” These factors include the concept that signal intensity is related to both driving pressure and volume flow rate, signal intensity varies with gain settings, the CW Doppler beam may not encompass the entire MR orifice area, and the impact of other machine settings is unknown.
The Education in Heart article in this issue (see page 244) discusses the management of pregnant women with prosthetic heart valves. In women with bioprosthetic valves, there is concern that pregnancy may accelerate structural valve deterioration, although this remains controversial. In women with MHVs, maternal mortality is high (1 to 15% in different series) with the major issue being management of anticoagulation to ensure prevention of valve thrombosis or systemic emboli in the mother while avoiding adverse fetal effects. This article reviews the background, evidence and recommendations for anticoagulation during pregnancy in women with MHVs and the approach to treatment of mechanical valve thrombosis.
The Image Challenge question (see page 189) shows an unusual cystic structure in the Heart. After reviewing the question and answer, you are sure to recognize this finding should you encounter it in your clinical practice.
Linked Articles
- Image challenge
- Education in Heart
- Editorial
- Editorial
- Arrhythmias and sudden death
- Editorial
- Valvular heart disease
- Valvular heart disease