Article Text

Abstract
Introduction Many conditions considered to be primary lung diseases are independently associated with adverse cardiovascular outcome. Systemic inflammation and subsequent fibrosis are hypothesised mechanisms. However, beyond the mechanical impact on right heart, characterisation of myocardial involvement in lung disease remains limited.
We present a combined heart-lung MRI protocol which allows simultaneous interrogation of heart and lung structure and function.
Methods Protocol (1.5T Siemens Avanto) includes steady state free precession (SSFP) cine imaging of the heart (standard long and short axis views), followed by inspiration and expiration cine lung imaging (sagittal planes). T2 prepared SFFP and T1 MOLLIE images are acquired in standard cardiac planes and left and right lungs.
Dynamic contrast enhanced MRI (DCE-MRI) sequences are performed using free breathing 2D saturation-recovery FLASH dynamic acquisitions in four planes (two LV short axis slices, left and right lung sagittal slices) with temporal resolution equal to 50% of patient’s heart rate. Three boluses of gadolinium contrast (dotarem) are administered: 0.005 mmol/kg, followed by 2 min of dynamic acquisitions; 0.05 mmol/kg followed by 6 min of dynamics; final dose of 0.1 mmol/kg.
Finally, late enhancement imaging and post-contrast T1 mapping are performed. Overall each scan protocol lasted for approximately 60 min.
Results Parametric mapping and LGE imaging provides direct tissue characterisation.
Myocardial and lung contrast agent kinetics are modelled from the DCE images in matlab (Extended Kety Model) to determine heart and lung capillary permeability (Ktrans), extracellular volume (ECV) and plasma volume fraction (vp). Regions of interest are drawn in the LV and RV cavities to obtain arterial input functions (AIF). The low dose AIF is multiplied by a factor of ten and the first pass peak is combined with the high dose AIF curve in order to correct for saturation effects (Figure 1).
Conclusions This combined heart lung protocol is an efficient and comprehensive imaging tool for simultaneous myocardial and pulmonary assessment. It has a potential to help elucidate complex links between pulmonary and myocardial pathologies, and is a model for other dual organ parametric MR imaging.

LV arterial input function (AIF); LD – low dose dotarem (0.005mmol/kg), HD – high dose dotarem (0.05 mmol/kg) Part A: Before merging of the curves. Part B: After merging of the curves.

Myocardial extracellular volume map.

{kind=link}
{kind=link}
{kind=link}
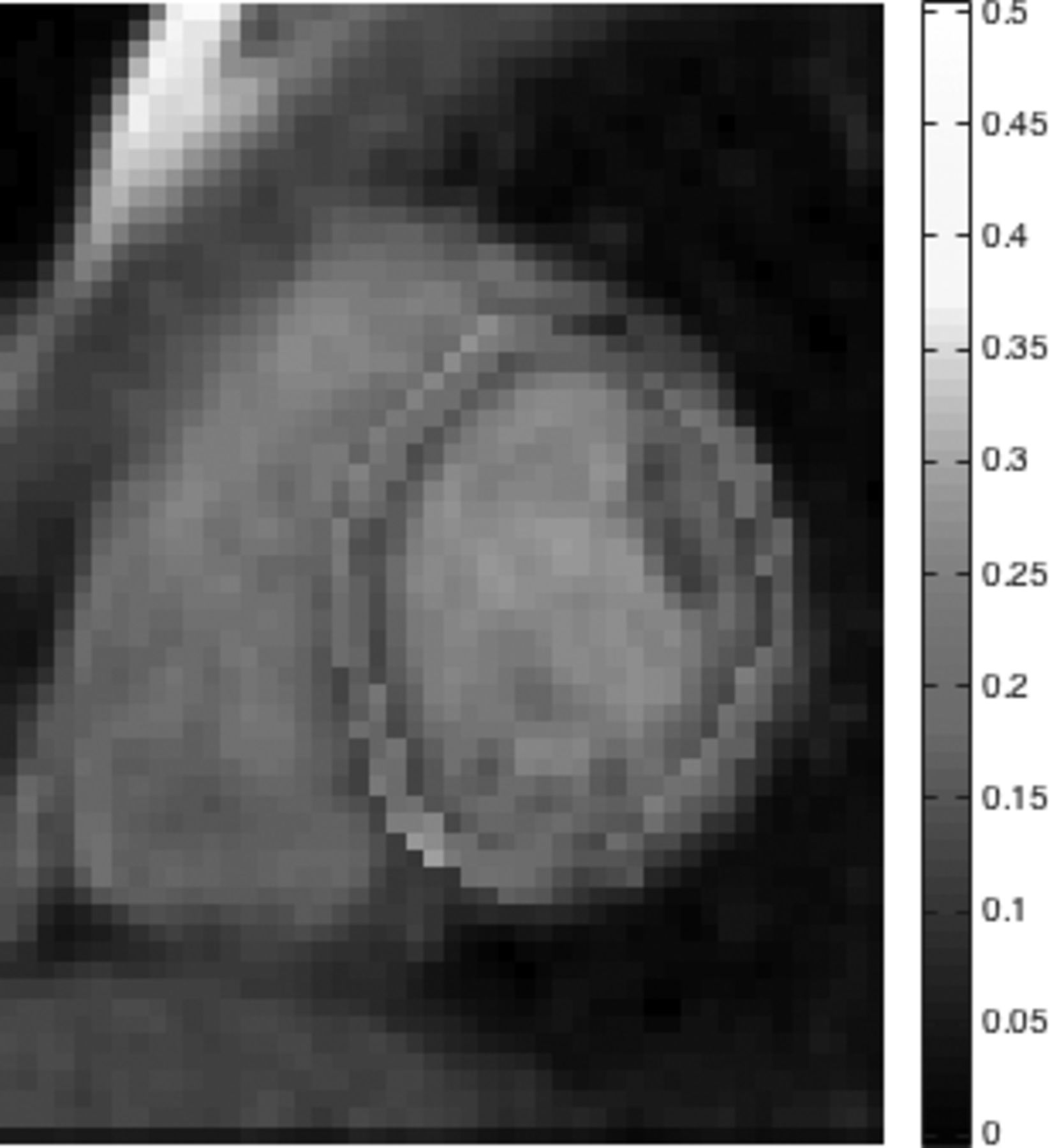
Lung extracellular volume map.