Article Text

Abstract
Interventricular septal haematoma is a rare postoperative complication in congenital heart surgery. We present one case of a 6-month-old after tetralogy of Fallot repair and 1 case of a 10-month-old after ventricular septal defect repair. Both were noted to have interventricular septal haematoma on intraoperative transoesophageal and postoperative echocardiogram. Although multiple previous reports, mainly in adults, have suggested aggressive intervention, both these cases were managed conservatively, highlighting the management and evolution of a rare postoperative complication in the paediatric population.
Case one Following antenatal diagnosis of tetralogy of Fallot (ToF), an infant with absent cerebellar vermis underwent elective repair at 6 months of age. Physical examination revealed a harsh pulmonary ejection systolic murmur, mild respiratory distress with oxygen saturations 93% and no hepatomegaly.
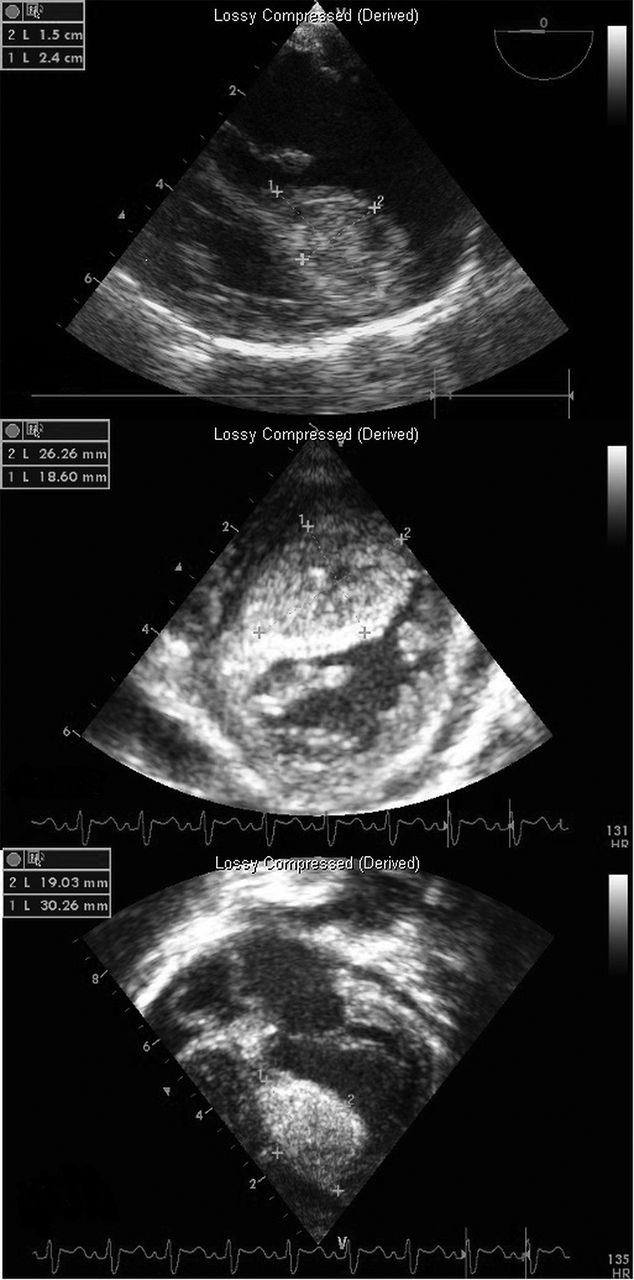
The repair was performed via a transatrial approach. The ventricular septal defect (VSD) was a large anteriorly malaligned perimembranous outlet type, closed with a bovine pericardial patch using 6/0 running prolene suture, reinforced with pledgeted 6/0 sutures. The Patent Foramen Ovale was closed directly and the hypoplastic pulmonary valve annulus was dilated using a 10 mm Hegar dilator. Transoesophageal echocardiogram (TOE) showed no residual VSD, no right ventricular outflow tract obstruction but a significant haematoma (Figure 1A) in the septum. Despite its size, a decision was made for a conservative approach in view of excellent surgical result and haemodynamic stability.
Transthoracic echocardiogram (TTE) that evening showed the interventricular septal (IVS) haematoma to be essentially unchanged in size with no inflow or outflow tract obstruction. Serial TTEs measured the haematoma to be at its largest 26×18 mm in short-axis view (Figure 1B) and 30×19 mm in 4-chamber view (Figure 1C). ECG demonstrated first-degree heart block. MDT discussion concluded that no intervention was needed as the infant remained haemodynamically stable
The postoperative course was uneventful, and serial TTEs confirmed reduction in size of the septal haematoma. The patient was discharged on Day 8 in sinus rhythm with right bundle branch block.
At follow-up 1 month later, there was no clinical concern and TTE demonstrated improved biventricular systolic function with a small residual VSD at the superior margin of the patch. A cystic lesion (4.5×4.5 mm) was present in the same position as the original haematoma, suggestive of false aneurysm into which there was arterial flow.
Case two A 10-month-old infant underwent elective repair, following postnatal diagnosis of VSD and mild mitral valve regurgitation. Examination confirmed normal heart sounds with a harsh pansystolic murmur loudest at the left lower sternal border with no respiratory distress and no hepatomegaly.
The defect was a moderate size perimembranous VSD partially covered by the septal leaflet of the tricuspid valve. It was closed with a bovine pericardial patch and 6/0 surgilene running suture. This was supported with a piece of autologous pericardium on the tricuspid valve septal leaflet. An additional two interrupted 6/0 pericardial sutures were placed to secure the patch in position. The infant came off bypass smoothly in sinus rhythm.
No TOE was performed; however, postoperative TTE showed no residual VSD with good ventricular systolic function and an IVS haematoma measuring 11×25 mm. Repeat TTE the following day showed the septal haematoma resolving and less echogenic in appearance. The patient remained haemodynamically stable with no rhythm disturbance and was discharged on Day 6 postoperatively.
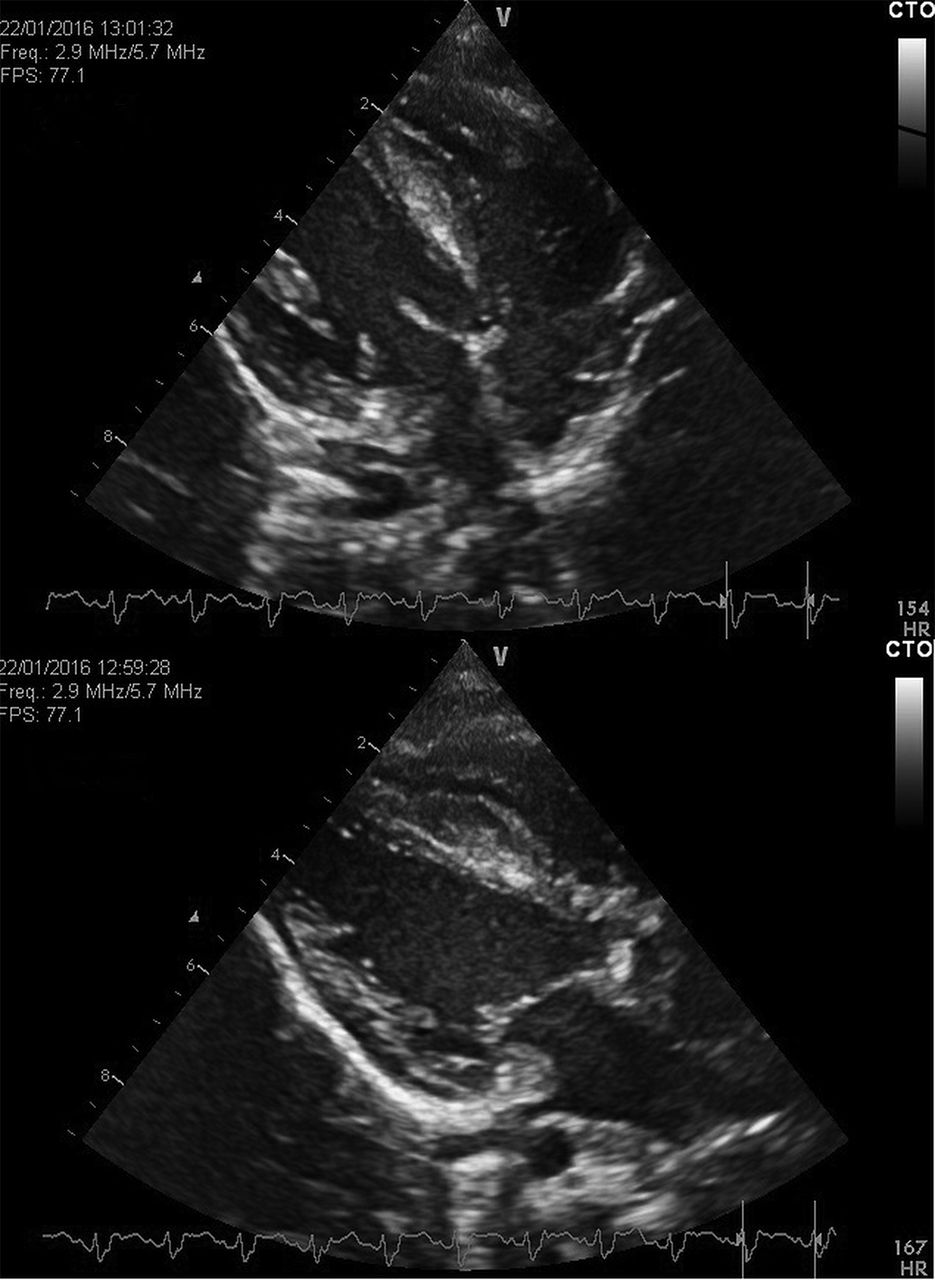
On follow-up a month later, he was clinically well; the echocardiogram showed the haematoma had significantly reduced in size (Figure 2A and B). Unlike the previous case, there was cystic collection, and follow-up was arranged for 6 months.
Discussion Haemorrhagic dissection of the IVS after patch closure of a VSD is a rare complication.1 This is the first report of a case where the haematoma was seen in a patient following ToF repair.
{kind=link}
{kind=link}
In both cases, we have described a rapid postoperative increase in the diameter of the IVS which suggests surgical trauma of the coronary septal branch during placement of the septal patch sutures. Anticoagulated, the bleeding probably dissects along a plane beneath the endocardium, resulting in a haematoma that bulges into the ventricular cavity,2 confirmed by echolucency on postoperative echocardiogram. Follow-up echocardiogram in Case 1 lends support to this theory with coronary flow seen in the cystic lesion within the resolving septal haematoma which likely dissipates into a ventricle.
Most reports are in the adult population where IVS haematoma has been described after myocardial infarction, percutaneous coronary artery intervention and coronary artery bypass grafting.2 The use of intraoperative TOE is essential in congenital heart surgery to facilitate the early detection of any complications.2,3 Haemodynamic instability dictates management with prompt reintervention, carried out in those cases with compromise through surgical drainage4,5 or with needle puncture.1 The vast majority of adult cases opt for aggressive intervention, thereby potentially influencing decision-making in paediatric cases following surgery.
Myocardial haematoma formation may cause haemodynamic instability or conduction abnormalities that may lead to serious short-term complications, including heart block, outflow obstruction and tamponade.3 Conservative approach is rarely adopted; however, in haemodynamically stable cases, complete and spontaneous resolution of the haematoma has been seldom demonstrated.2,4
Management is dictated by initial presentation, ECGs are mandatory initially to ensure no AV block and as the haematoma resolves, we feel it is unlikely to result in later AV nodal issues. In the absence of haemodynamic instability, echocardiography remains the mainstay of follow-up.
References
Padalino M, Speggiorin S, Pittarello D, et al. Unexpected interventricular septal hematoma after ventricular septal defect closure: Intraoperative echocardiographic early detection. Eur J Echocardiogr2007;8:395–398.
Eyileten Z, Aliyev A, Çiftçi O, et al. An extremely rare complication of congenital heart surgery: interventricular septal hematoma. Turk J Pediatr2013;55:662–664
Mart C, Kaza A. Postoperative dissecting ventricular septal hematoma: recognition and treatment. ISRN Pediatr2011:534940.
Jensen R, Burg P, Anderson C, et al. Posttoperative ventricular septal hematoma: Natural history of two paediatric cases. J Thorac Cardiovasc Surg2007;133:651–1652.
Drago M, Butera G, Giamberti A, et al. Interventricular septal haematoma in ventricular septal defect patch closure. Ann Thorac Surg2005;79:1764–5.