Article Text

Abstract
Introduction Initiation of reentrant ventricular tachycardia (VT) involves complex interactions between activation (AT) and repolarization times (RT). Recently, an algorithm has been developed to generate a spatial map (designated the re-entry vulnerability index-RVI) from intervals between local ATs and RTs at adjacent points over a multielectrode grid. The algorithm has been shown to accurately identify the region of a macro-reentrant circuit in two animal models (1). The aim of this study was to test the feasibility of RVI mapping in the right ventricle (RV) to aid ablation strategy of reentrant arrhythmias.
Methods Patients with Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC) (n=10), Brugada Syndrome (BrS) (n=14) and normal heart RV outflow tract (RVOT) VT (n=6) underwent electrophysiological studies and were followed up for 113±21 months post procedure. Unipolar electrograms were recorded from a non-contact array (St Jude Medical) placed in the RVOT and geometry created with the Ensite system. Recordings were made during a programmed electrical stimulation protocol consisting of a 600 ms drive train and S2 extras. ATs and RTs were computed from the unipolar electrograms and the RVI calculated as previously described (1). Minimum 10% of global RVI values corrected for cycle length (RVIc10% ) and distance between region of lowest 5% of RVI values and region of earliest activation during VT (Dmin ) were computed for each patient.
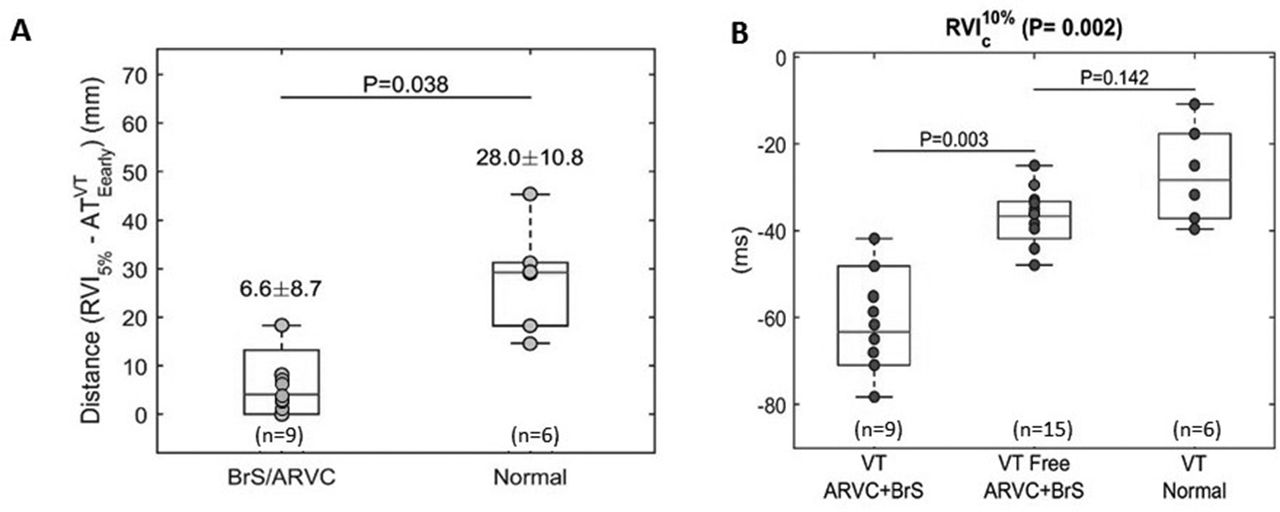
Results Shortest values of RVI, which represent sites of highest susceptibility to re-entry, co-localised with earliest activation point during VT in the 9 patients with ARVC/BrS where VT was initiated (figure 1). In the ARVC patients this corresponded with location of RV scar as seen on MRI. In the 6 patients with normal heart focal VT, regions of lowest RVI did not co-localise with VT origin. Distance between region of lowest RVI and region of earliest activation during VT, Dmin , was significantly lower in BrS and ARVC than in normal heart VT (Fig 2A). In both ARVC patients Dmin =0, indicating region of lowest RVI overlapped with region of earliest VT activation.
Of the patients with ARVC/BrS, those with inducible VT or clinical VT at follow-up had significantly lower minimum values of RVIc than those without (−61.0±13.8 ms vs −37.1±7.1 ms) (Fig 2B). Patients with normal heart VT had highest values of RVIc (−27.0±11.3 ms).
Conclusion An algorithm based on relative local ATs and RTs identifies localised regions of high susceptibility to conduction block and re-entry, with lowest RVI values localising VT origin of reentrant but not focal arrhythmias.
This index could be applied to:
1. Risk stratify ARVC/BrS patients to target ICD prophylaxis.
2. Target ablation for reentrant arrhythmias which are difficult to induce or are haemodynamically unstable, without need for arrhythmia initiation.
Reference
. Child Net al. Heart Rhythm2015;12:1644–1653

{kind=link}
{kind=link}
- ventricular arrhythmia
- risk stratification
- ablation