Article Text

Abstract
Introduction Persistent AF (PeAF) ablation continues to be a challenge, primarily because the mechanism of AF is not clearly defined and even when successfully ablated may evolve into multiple atrial tachycardias or flutters (AT/AFl) during the course of a procedure. Sequential mapping with existing 3D mapping systems can make procedures long and complex. We report the use of a novel simultaneous non-contact ultrasound (US) imaging and mapping system (AcQMap) to characterise of AT/AFl during PeAF ablation.
Methods The AcQMap system consists of a basket catheter (48 US transducers, 48 electrodes) which simultaneously acquires 100,000+ US points/min to reconstruct chamber anatomy and 1 50 000 intracardiac unipolar voltage points/s to map cardiac activity. The 3D surface is algorithmically reconstructed from the US point-set with mesh-density comparable to a segmented CT.1 Inverse and forward algorithms are applied on intracardiac voltage to derive and display electrical activation as dipole density™ (DD) and unipolar voltage maps respectively, upon the US-constructed 3D anatomy.
Results Data were collected from three patients booked for a first PeAF ablation (2 male, age 48±13 years, time in PerAF 1.7±1.2 years) who also demonstrated AT/AFl either before or during the procedure. All patients had previously failed DCCV and were receiving amiodarone. The AcQMap system was used to measure cardiac voltage, apply its DD algorithm and display electrical activation on the US constructed 3D anatomy to demonstrate the AFl/AT circuit. The circuit was validated using contact mapping and response to ablation. Left atrial (LA) and (right atrial) RA surface acquisition times were 296±20 s and 209±88 s respectively.
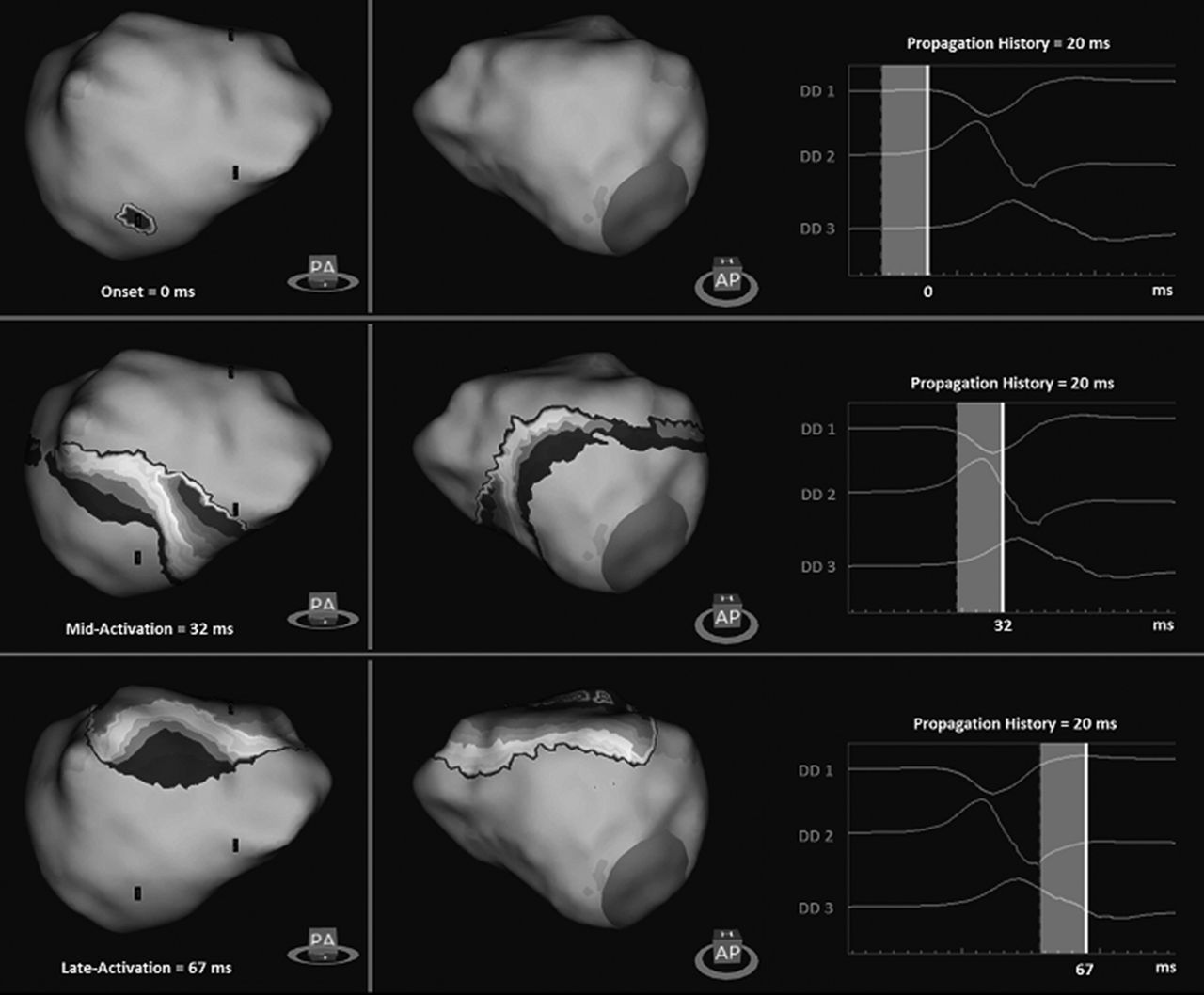
The maps demonstrated a macro-reentrant circuit in all patients and were used to guide ablation at the isthmus of the circuit. Procedural end point was bidirectional block. Patient 1 presented in typical right AFl (figure 1); Patient 2 presented in SR but with an easily inducible AT around the right upper PV; Patient 3 presented in AF which organised to an AT around the LA posterior wall, and after ablation and termination of this, subsequently to a typical right AFl. Figure 2 shows a Dd-based isochronal plot of the initial AT activation sequence from Patient 3, with breakout at the inferior aspect of the LA posterior wall. All AT/AFl terminated during formation of the ablation line. Maps were then created in SR, and during pacing to demonstrate bidirectional block.
Conclusions Real-time US and DD based LA and RA reconstructions using the AcQMap system provide high resolution electro-anatomical maps, allowing rapid and accurate targeting of critical isthmuses for ablation of macro-reentrant AT/AFl. This technique also raises the possibility of mapping AF with more precision to identify areas of interest as potential ablation targets.
Reference 1. Heck PM et al. Europace 2015;17(s5):6–9.

{kind=link}
{kind=link}
- Atrial arrhythmia
- Mapping
- Technology