Article Text

Abstract
Introduction Prolonged ECG monitoring is an increasingly advocated method to detect silent AF and other arrhythmias. Inevitably, the wider use of prolonged ECG monitoring will yield unexpected and serious findings requiring swift action. Here, we report the diagnostic yield of 7 day Holter ECG monitoring requested through primary and secondary care. We also highlight the clinical and Holter ECG parameters associated with new AF.
Methods We analysed all 7 day Holter ECG tests in Sandwell and West Birmingham NHS Trust from 1st April 2014 to 30th April 2016, using Spacelabs Sentinel server running Pathfinder V 1.7.1. Tests were bookable by primary care and hospital physicians. Holter recordings from 364 patients, previously reported by cardiac physiologists were reviewed by physicians trained in Holter analysis. 46 patients had previously diagnosed AF and were excluded from the analysis. Here we present the results from a final cohort of 318 patients.
Results Mean age of the patients was 59.2 years (median 56 years, IQR 43–72) and 55% were male. Average time of monitoring was 162.2 hours. Palpitations (56%), dizziness (16%), ischaemic stroke or TIA (15%), syncope (10%), and chest pain (3%) were reasons for referral. New AF was diagnosed in 25/318 patients. The pick-up rate of incidental AF was 7.86%. 9/48 (18.7%) of patients with CVA and 16/178 (8.9%) with palpitations had new AF. For 7 day Holters performed with intention to look for AF (stroke and palpitations) the combined diagnostic yield to pick up new AF was 11%. There was no AF detected for indications of dizziness, syncope or chest pain.
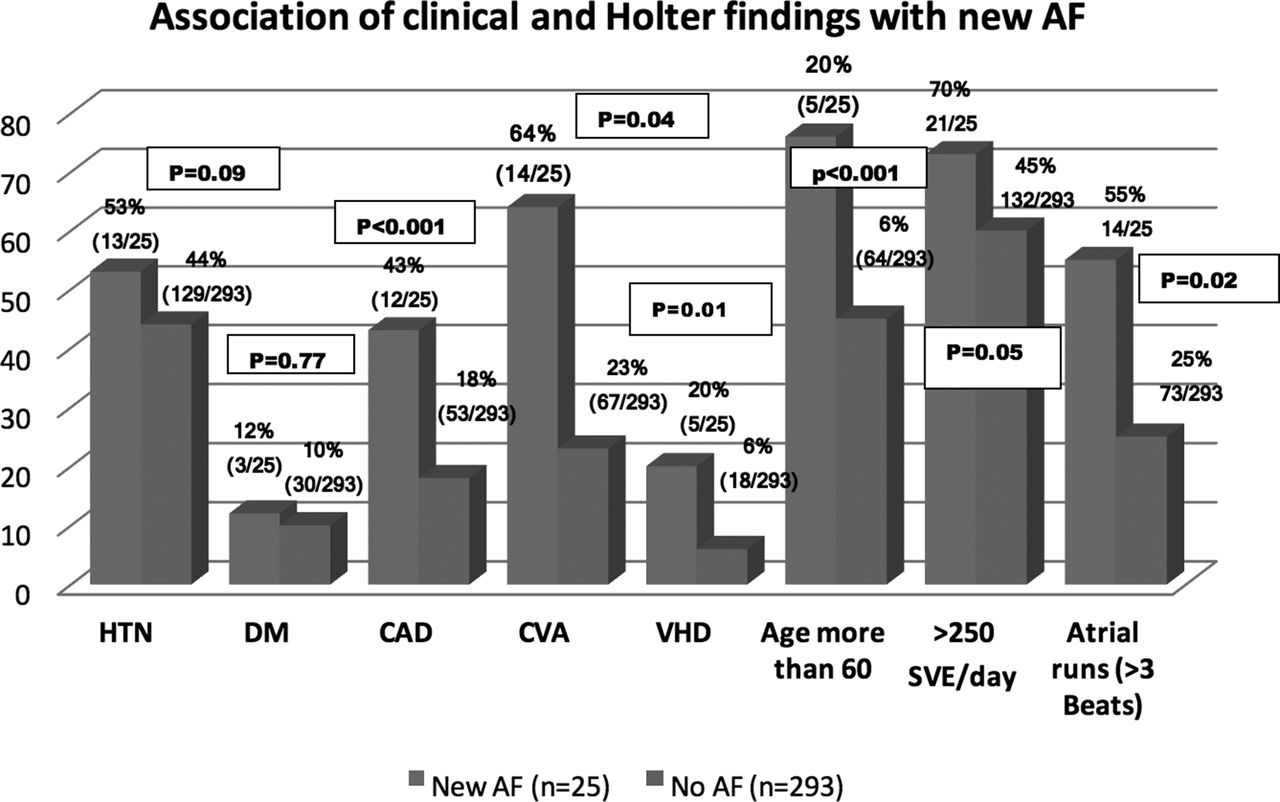
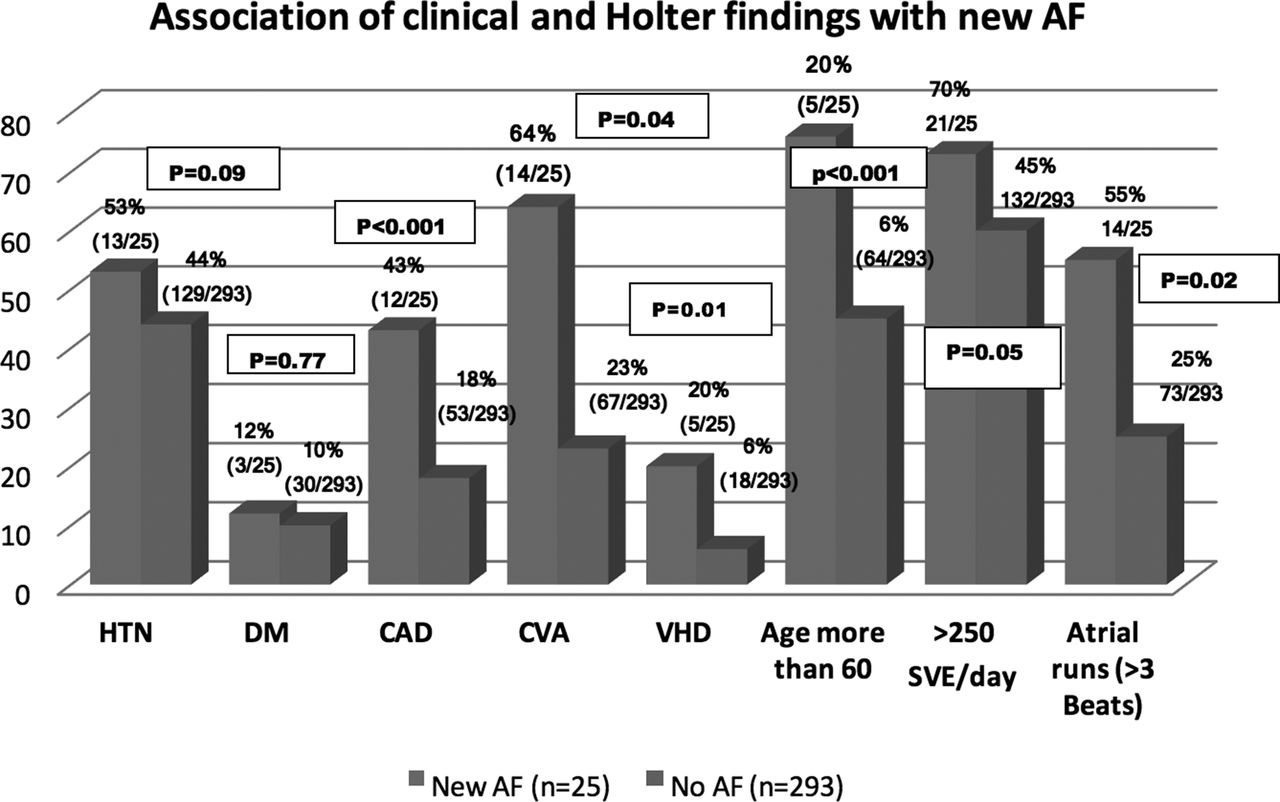
Patients with newly diagnosed AF were older with mean age 71 years (CI 66–78, SD 17.3) vs. 57 years (CI 55–59, SD 17.6) for non-AF group (p=0.001), more often suffered from coronary artery disease (43% vs 18%, p=0.001), prior stroke or TIA (64% vs 23%, p=0.04), moderate to severe valvular heart disease (20% vs 6%, p=0.01), had higher occurrence of >250 supra ventricular ectopics/day (73% vs 60%, p=0.05) and atrial runs of more than 3 beats (55% vs 25%, 0=0.002 respectively). Heart rate parameters for patients with and without AF were not different in our cohort. Other medically relevant findings were 2nd degree AV block (9/318, 2.8%), 3rd degree AV block (2/318, 0.6%) and non-sustained VT (11/318, 3.4%).
Conclusions Prolonged ECG monitoring in a real life cohort, especially in patients with high risk of AF, leads to higher diagnostic yield, with significant therapeutic consequences. It appears reasonable to provide open access to prolonged ECG monitoring to at-risk populations in primary and secondary care. Further analysis of risk factors for paroxysmal AF and systematic evaluations of treatment and outcomes after AF screening are warranted to define populations for screening for silent AF.
{kind=link}
- atrial fibrillation
- ECG
- Holter monitoring