Article Text

Abstract
Introduction Effort tolerance is impaired in end stage kidney disease. Peak oxygen uptake (VO2peak) has been shown to be a powerful predictor of survival in haemodialysis patients. A low VO2peak and percent predicted VO2 at the anaerobic threshold (VO2 AT) have also been associated with excess mortality in patients undergoing kidney transplantation. Data on effort tolerance and cardiovascular disease in early chronic kidney disease (CKD) are very sparse though it is well recognised that cardiovascular mortality begins to increase at a glomerular filtration rate (eGFR) of about 75ml/min/m2.
Methods This study examined effort tolerance, cardiac structure and function in 60 patients with CKD (stages 2 to 5) without known cardiovascular disease or diabetes. All patients underwent a cardiopulmonary exercise bicycle test using an individualised ramp protocol. Myocardial ischaemia was excluded by exercise stress echocardiography or 99m technetium tetrofosmin single photon electron computed tomography. Lung disease was excluded by formal lung function testing. Cardiac magnetic resonance imaging without gadolinium contrast was used to assess cardiac function and structure. The Kruskall Wallis test was used to compare the difference in mean values across stages of CKD. Correlation coefficients were measured to look for trends between continuous variables.
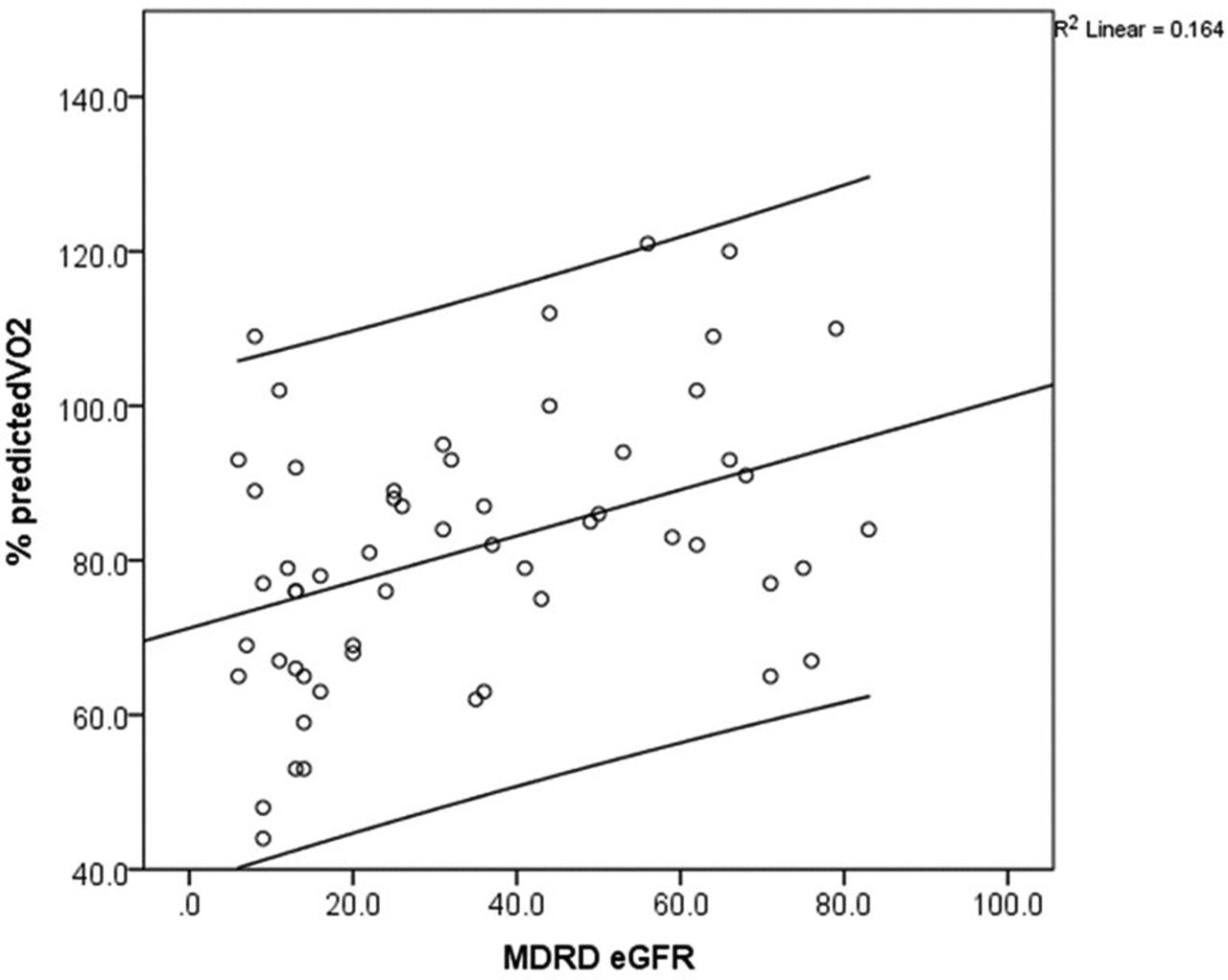
Results Table 1 shows the baseline characteristics per CKD stage. Percent predicted peak VO2 was negatively associated with eGFR (r=−0.358, p=0.007) even after correction for age and haemoglobin (p=0.005). NT pro-BNP was negatively associated with eGFR (r=−0.586, p=0.001), even after similar correction (p<0.001). The percent predicted VO2 at the anaerobic threshold was also negatively associated with worsening eGFR (r=0.282, p=0.039). Exercise capacity (VO2 AT) was negatively associated with increasing LV mass (r=−0.382, p=0.006) but there was no significant association with left ventricular (LV) size, ejection fraction or global longitudinal strain.
Discussion and implications Effort tolerance falls from the earliest stages of CKD in association with a progressive increase in LV mass and NT pro-BNP. This is the first study to examine exercise capacity in patients with early stage CKD in whom coronary artery disease has been excluded, and further study is needed to confirm whether the reduction in exercise capacity is a reflection of diastolic impairment and myocardial fibrosis that characterise end-stage kidney disease.
Baseline demographics across each stage of CKD

{kind=link}
The association between eGFR and% predicted VO2. Lines represent the line of best fit and 95% confidence intervals.
- Subclinical heart disease
- Cardiopulmonary exercise testing
- chronic kidney disease