Article Text

Abstract
Background In over 50% of patients with angina, the underlying ischaemia is related to microvascular dysfunction (MVD), rather than epicardial coronary artery disease (CAD). Clinically, MVD remains a major diagnostic challenge, which hinders targeted therapy and confers impaired clinical outcomes. Myocardial perfusion reserve (MPR), as assessed by cardiovascular magnetic resonance (CMR), is impaired in those with microvascular angina. We sought to objectively diagnose microvascular ischaemia using CMR by defining an MPR cut-off, validated against invasive coronary microvascular physiology (Index of Microvascular Resistance, IMR).
Methods 75 subjects (50 patients with angina and suspected CAD; 25 healthy controls) underwent CMR to assess LV function, MPR (adenosine stress/rest first-pass perfusion imaging) and viability (late gadolinium enhancement). All patients underwent invasive coronary angiography with pressure-wire assessment of IMR and fractional flow reserve (FFR). A total of 120 coronary arteries were assessed. CMR images were analysed by observers blinded to clinical and angiographic data. MPR was defined as the ratio of stress/rest myocardial signal intensity upslope gradients during gadolinium first-pass perfusion imaging, normalised to LV blood pool enhancement. Infarcted myocardium was identified using LGE and excluded from analysis.
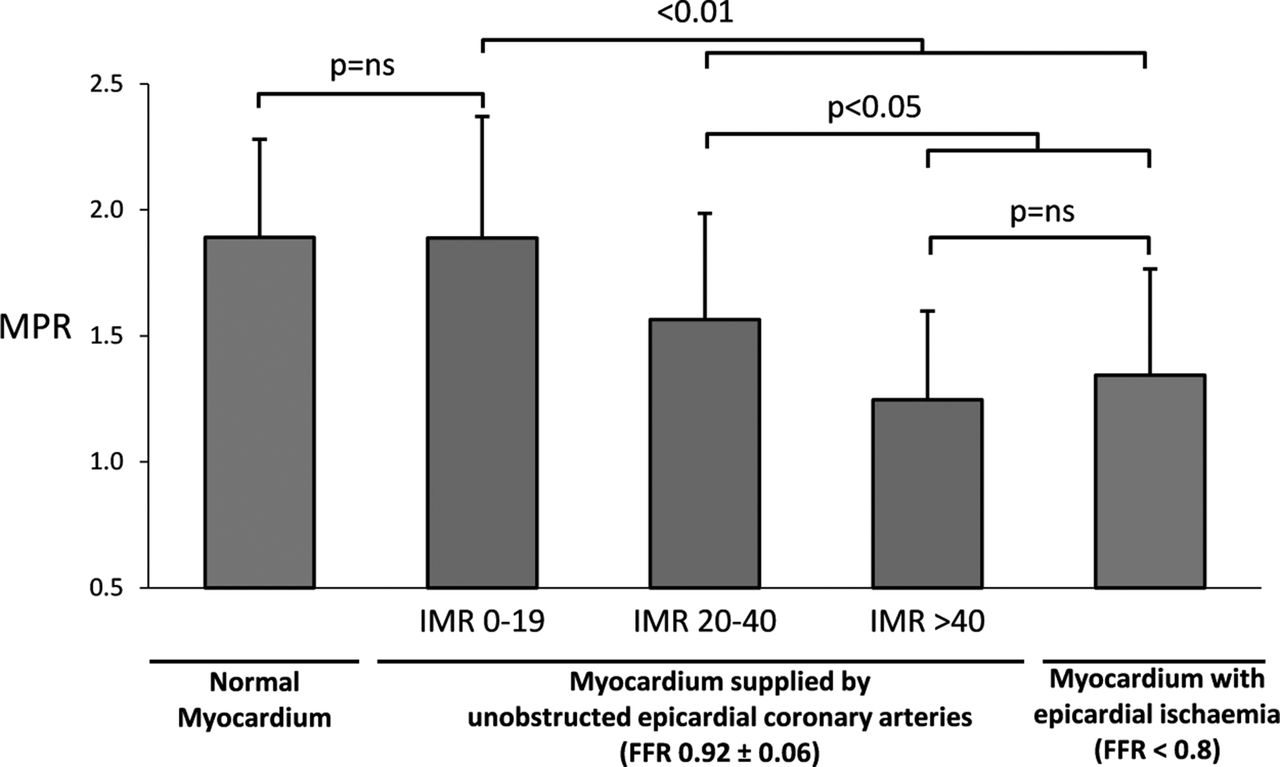
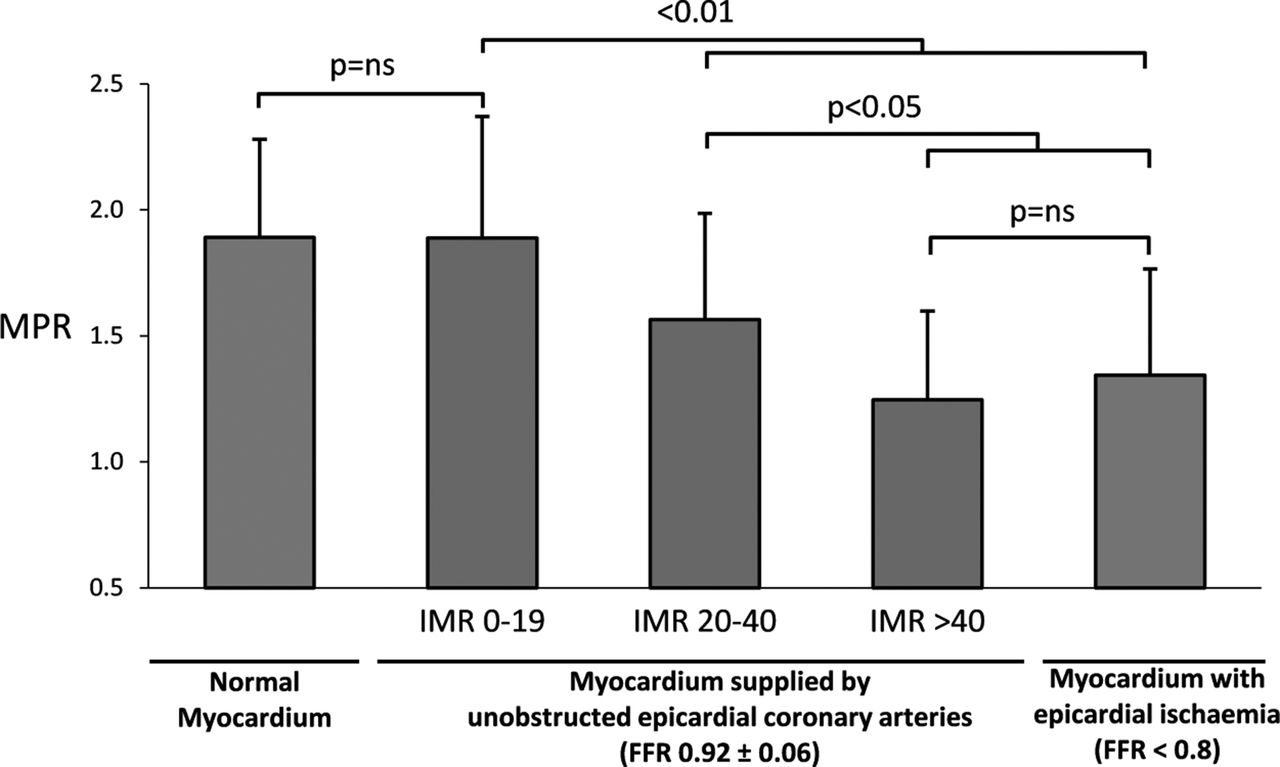
Results For reference, myocardium downstream of significant epicardial stenosis (FFR<0.8) had lower MPR than healthy controls (1.3±0.4 vs 1.9±0.4, p<0.001, figure 1). Downstream of unobstructed epicardial coronary arteries (FFR>0.8), non-infarcted myocardium had intermediate MPR: (unobstructed-CAD 1.6±0.4, obstructed-CAD 1.3±0.4; controls: 1.9±0.4, p<0.001 by ANOVA). When further stratified by IMR, myocardium with IMR<20 had comparable MPR to normal controls (1.9±0.5 vs 1.9±0.4, p=0.98); as IMR increased, there was progressive reduction in MPR (IMR<20: 1.9±0.5, IMR20-40: 1.5±0.4, IMR>40: 1.3±0.4; all p<0.01 by ANOVA). Myocardium with high IMR>40 but unobstructed epicardial coronary arteries had equivalent MPR to ischaemic myocardium supplied by significant epicardial stenosis (1.3±0.4 vs 1.3±0.4, p=0.48, figure 1). Downstream of unobstructed epicardial coronary arteries of CAD patients, MPR 1.5 detected microvascular ischaemia (defined by IMR>40) with a sensitivity of 82%, specificity of 83%, and accuracy of 83% on ROC analysis (AUC 0.87±0.06, figure 2).
Conclusions Microvascular ischaemia can be objectively diagnosed using CMR perfusion imaging. Reduced MPR is related to increased microvascular resistance, as validated by invasive IMR. The novel MPR criterion of 1.5, to detect high IMR>40, can confirm the clinical diagnosis of microvascular ischaemia, enabling targeted therapy and disease monitoring.
{kind=link}
In myocardium downstream unobstructed epicardial coronary arteries, myocardial perfusion reserve (MPR) decreases as index of microvascular resistance (IMR) increases. Myocardium with high IMR>40 had equivalent MPR to ischaemic myocardium supplied by significant epicardial stenosis. Bars represent mean±SD. FFR = fractional flow reserve.
- Microvascular ischaemia
- CMR
- IMR