Article Text

Abstract
Introduction Assessment for pulmonary arterial hypertension (PAH) is a common indication for transthoracic echocardiogram (TTE). PAH is defined as a mean pulmonary artery pressure (PAP)>25 mmHg and is associated with reduced quality of life, increased mortality and morbidity. TTE is the major technique for screening and serial assessment. The general consensus amongst cardiologists at this unit is that there is poor agreement between reported echo values and invasively derived measures at right heart catheter (RHC). The primary aim of this study was to complete a retrospective analysis directly comparing TTE estimation of right heart pressures with those measured invasively at RHC for:
1. Pulmonary artery systolic pressure (PASPP)
2. Mean pulmonary artery pressure (MPAP)
3. Right atrial pressure (RAp)
4. Other echocardiographic features of pulmonary hypertension and the presence of raised pulmonary pressures on RHC
Method Data was collected from patients attending for RHC between 01/01/2015 and 30/09/2016, who had both RHC and TTE within 3 months.
Age, height and weight were recorded.
Invasive and echo derived measurements were re-analysed by a senior, BSE accredited cardiac physiologist for PASP (4VÃ,² + Rap), MPAP (0.61 * PASP+2), RAp (IVC:<2.1 cm with normal respiratory variation Rap=5 mmHg, IVC>2.1 cm with <50% respiratory variation Rap=15 mmHg) and other echo features of PHTN: RV Size, RV function and presence of septal flattening.
Results 150 patients were listed for RHC, 34 (22%) also had TTE within 3 months. There were 16 male and 18 female subjects with a mean age 66 years.
21 (62%) patients had PHTN, diagnosed by MPAP>25 mmHg on cardiac catheter. Of those, echo subdivision showed 38% had mild (25–40 mmHg), 19% moderate (41–55 mmHg) and 43% severe (>55 mmHg) PHTN.
Invasive measurements were compared to the original echo report: 50% of patients with mild PHTN, 75% of patients with mod PHTN and 88% of patients with severe PHTN had other echocardiographic features associated with pulmonary hypertension.
There was no correlation between invasive and echo assessment or right atrial pressure (R2 0.003; Pearson Correlation 0.052, p=0.78).
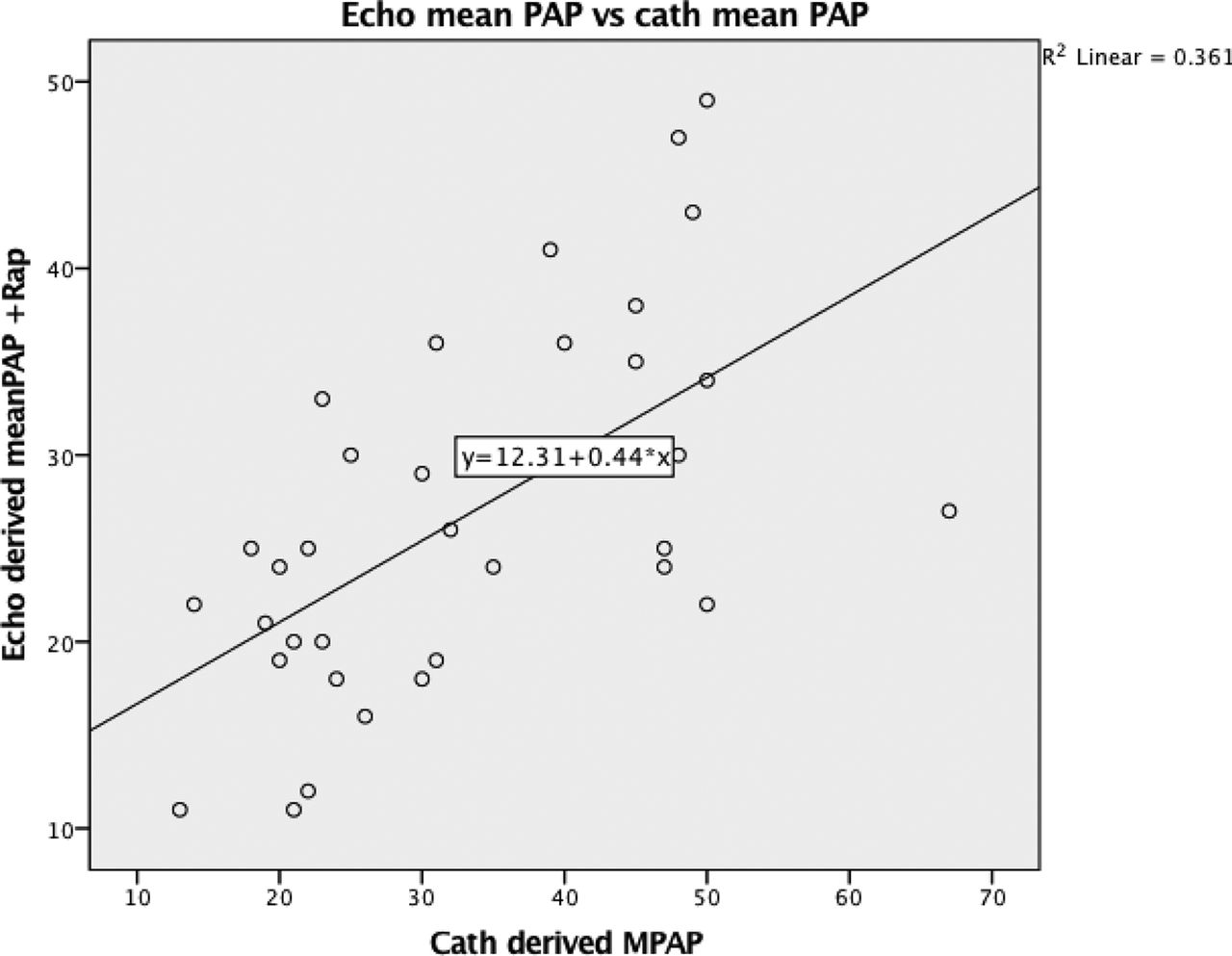
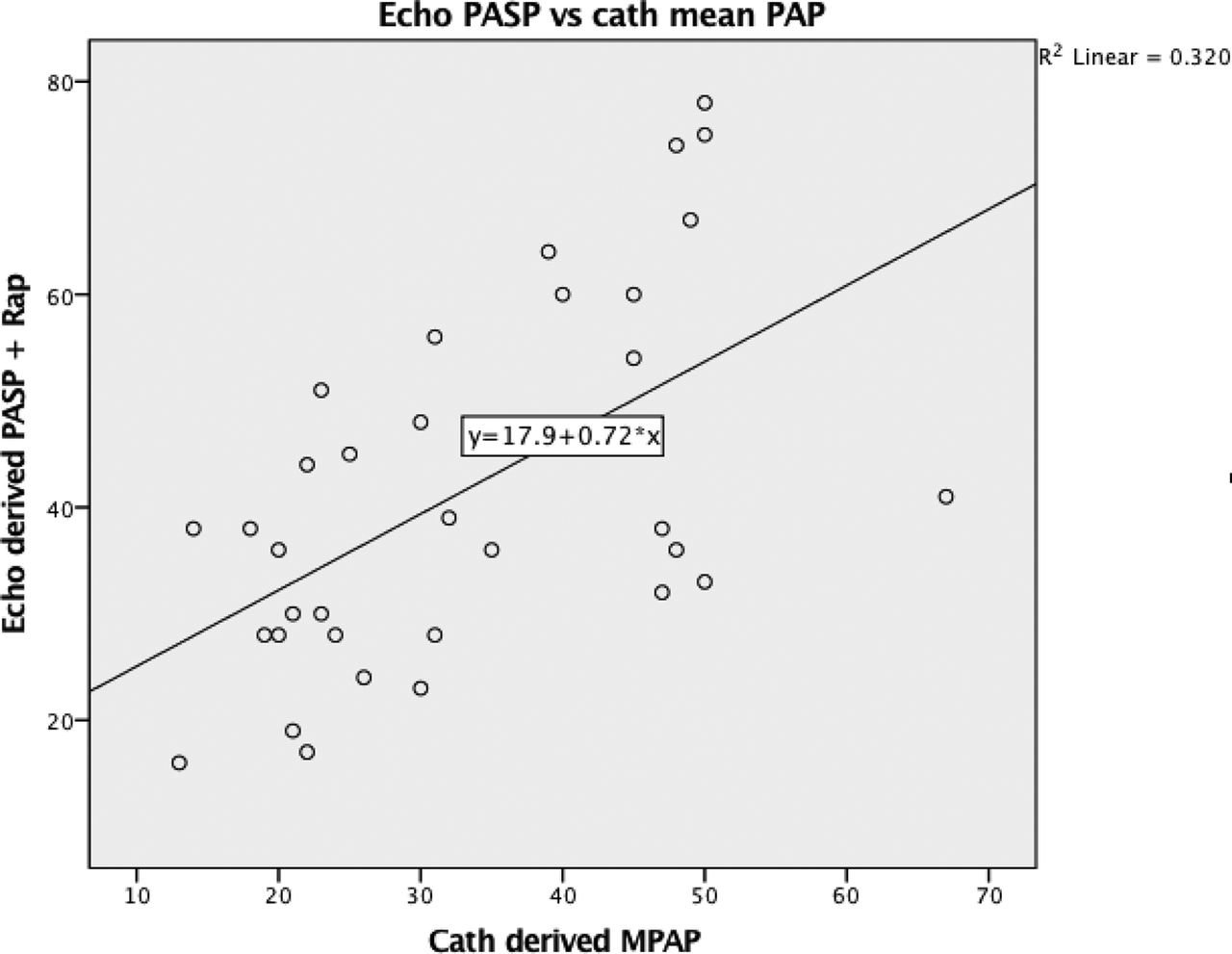
There was good correlation between RHC derived mean PAP and both echo mean PAP (R2 0.36; Pearson Correlation 0.60, p<0.01) and PASP (R2 0.32; Pearson Correlation 0.56, p<0.01).
The diagnostic equivalent of a mean RHC PAP of 25 mmHG was for a PASP 35.9 mmHG and a MPAP of 23.3 mmHg. Pulmonary artery systolic pressure being the most often reported in general echocardiographic reports in this institution.
Conclusion These results demonstrate that TTE derived measures of Rap correlate poorly with invasive measurements. However, this has no impact on the traditional calculations for mean PAP and PASP by echocardiography, which correlate well with the RHC data.

{kind=link}
{kind=link}
- pulmonary hypertension
- echocardiography
- right heart catheter