Article Text

Abstract
Background During low-dose dobutamine stress echocardiography (LDDSE) in low-flow low-gradient aortic stenosis (LFLGAS), both the aortic stenosis (AS) severity and the presence of contractile reserve (CR) are conventionally assessed based on stroke volume flow reserve (SVFR), which is defined as stroke volume [SV] increase 20%. However frequent exaggerated chronotropic response to dobutamine with shortening left ventricular time result in SV drop. On the contrary, transvalvular flow rate (FR) (SV/ejection time) and left ventricular ejection fraction (LVEF) may increase. We aimed to assess the value of FR 200 ml/s (normal FR) and LVEF change in the identification of true severe AS (TSAS) and the assessment of CR respectively.
Methods Accordingly 74 consecutive patients (mean age 78 years) with LFLGAS referred for LDDSE for determination of AS severity and CR underwent retrospective assessment of SV, FR, LVEF and standard echocardiographic parameters of AS severity (Table 1). The outcome assessed was all-cause mortality censored for aortic valve intervention.
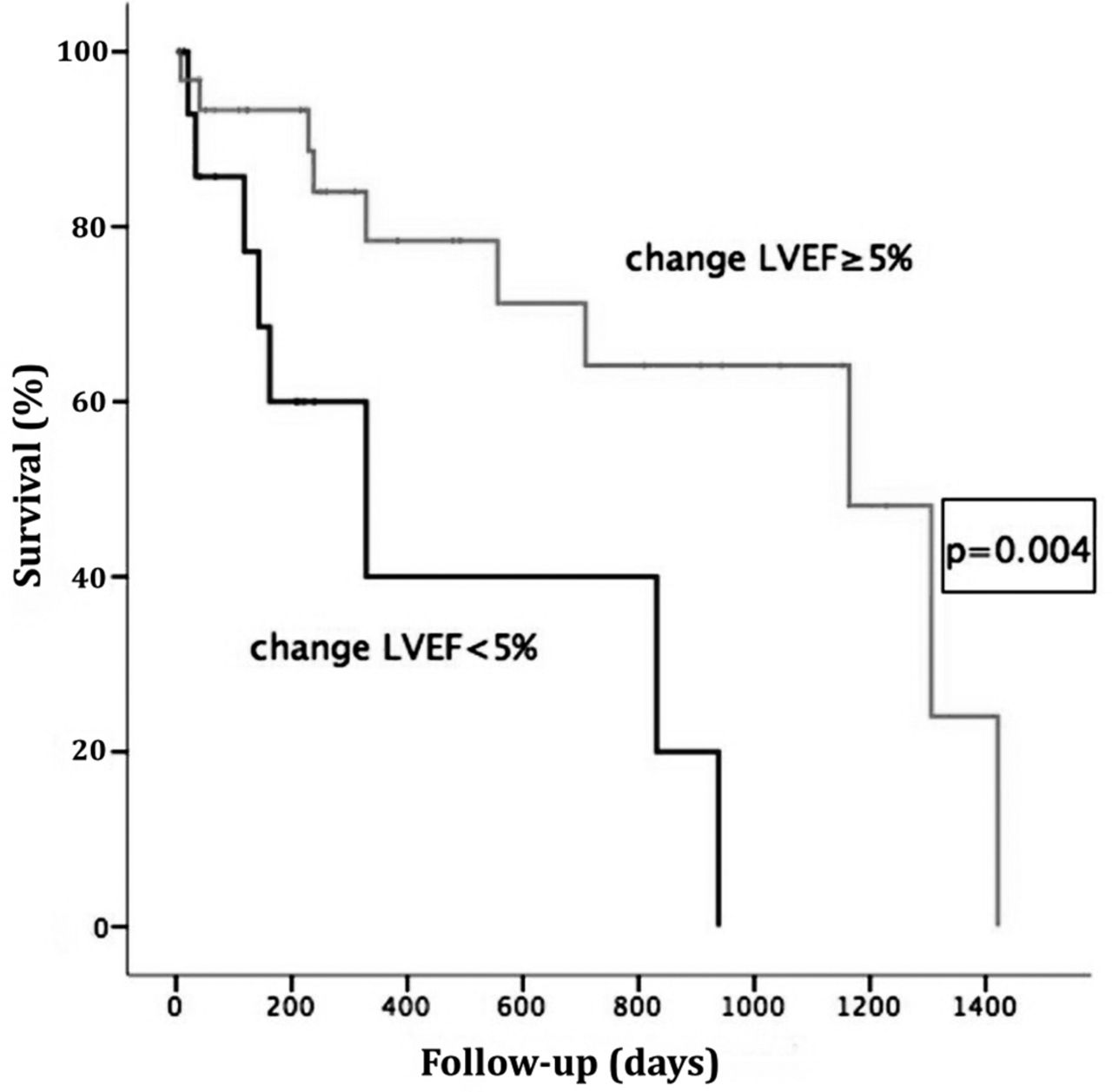
Results SVFR was present in 30 (40.5%) of the 74 patients whereas FR 200 ml/s was achieved in 60 (81.1%) (p<0.001). During the median follow-up of 316.5 days 28 (37.8%) deaths occurred. Amongst all standard echocardiographic predictors of AS severity at peak stress (aortic valve mean and peak gradient, peak velocity and area [AVA]) and clinical prognostic factors, AVA was an independent predictor of death (HR=0.1, 95%CI=0.02–0.7, p=0.03), and was therefore used to define TSAS (stress AVA 1.01cm2). TSAS was present in 47 (63.5%) patients of whom SVFR correctly identified 17 (36.2%) compared to 34 (72.3%) with FR 200 ml/s (p=0.001). In the 48 patients with LVEF 50%, amongst SV, FR and LVEF changes, only the latter was an independent predictor of death (HR=0.92, 95% CI=0.87–0.98, p=0.02) (Table 2). LVEF change of <5% was the best cut-off for the prediction of death (log rank p=0.004) and therefore for determination of CR (Figures 1-2). Increase in LVEF 5% had a significant impact on survival both on patients that underwent aortic valve intervention (log rank p=0.03) and those who underwent medical management (log rank p=0.01), as opposed to presence of SVFR (log rank p=0.234 and p=0.708 respectively).
Conclusions During LDDSE in LFLGAS normalised FR, not SVFR, is a better determinant of TSAS, whereas assessment of LVEF change instead of SVFR determines CR.
Patient echocardiographic characteristics
Univariable and multivariable analysis for prediction of all-cause mortality in patients with LVEF 50%

{kind=link}
{kind=link}
- low-flow low-gradient aortic stenosis
- low-dose dobutamine stress echocardiography
- contractile reserve