Article Text

Statistics from Altmetric.com
The cornerstone of treatment for patients with severe aortic stenosis (AS) is prompt valve replacement as soon as even mild symptoms are present. Even so, many patients are referred much later in the disease course, either because the primary care provider did not make the correct diagnosis or erroneously assumed the patient was ‘too old’ or ‘too sick’ to undergo valve replacement. In this situation, transfer to a heart valve centre often occurs only when the patient becomes haemodynamically unstable. Optimal emergency management of decompensated severe AS is controversial—attempts at medical stabilisation typically are futile, surgical risk is prohibitive and the decision to perform balloon aortic valvuloplasty (BAV) or transcatheter aortic valve implantation (TAVI) is not straightforward.
In this issue of Heart, Bongiovanni and colleagues1 report the outcomes of 141 patients with decompensated severe AS treated with TAVI (n=23) or BAV (n=118). Procedural mortality was 8.7% for TAVI compared with 20.3% for BAV with 30-day cardiovascular mortality rates of 23.8% for TAVI and 33.0% for BAV (figure 1). These differences are not statistically significant and were not affected by potential confounders. The subgroup of patients who underwent TAVI after an initial BAV (n=32) still had high procedural (9.4%) and 30-day (15.6%) mortality rates. Compared with BAV, TAVI was associated with more major vascular complications and strokes.

Kaplan-Meier survival curves for eBAV and eTAVI patients (restricted to the first 2 years of follow-up). The eBAV patients with subsequent elective TAVI were censored at the time of TAVI intervention. Corresponding Cox models were fitted. The estimated HR comparing eTAVI patients with eBAV is 0.59 (0.28; 1.25), P=0.169. The estimated HR is comparable following adjustment for age, logistic Euroscore, atrial fibrillation, coronary artery disease and a PCI in the 30 days preceding the emergency procedure: 0.45 (0.19, 1.08), P=0.074. eBAV, emergency balloon valvuloplasty; eTAVI, emergency transcatheter aortic valve implantation; TAVI, transcatheter aortic valve implantation.
In the accompanying editorial, Adamson and Cruden2 discuss the challenges of management in patients with decompensated severe AS. They emphasise that: “Central to this decision making is the multidisciplinary Heart Team through a careful and thorough assessment to evaluate whether aortic stenosis is the principal cause of decompensation, comorbid status, technical factors and prognosis.” However, they conclude: “where technically feasible, in carefully selected patients with minimal comorbidity and an otherwise favourable prognosis, a strategy of up-front emergency TAVI may be considered. For the majority of patients, however, BAV affords the opportunity to palliate symptoms, assess treatment response and clarify comorbid status and prognosis.” No doubt, this controversy is not yet over.
Among the many factors that predict longevity, one of the simplest to measure is resting heart rate (RHR), which is associated with a 30%–50% excess mortality for every 20 bpm increase in RHR. Although RHR depends partly on extrinsic factors, such as physical conditioning, there also is a heritable component. In a study of 4282 twins without cardiovascular disease, overall hereditability estimates were 0.23 (95% CI 0.15 to 0.30) overall; 0.27 (95% CI 0.15 to 0.38) for males and 0.17 (95% CI 0.06 to 0.28) for females.3 RHR was significantly associated with mortality, even after adjustment for potential cofounding variables, with an all-cause mortality hazard ratio of 1.56 (95% CI 1.21 to 2.03) and a cardiovascular mortality hazard ratio of 2.19 (1.30 to 3.67) for a RHR of >90 compared with 61–70 bpm.
The association between RHR and mortality and previous smaller studies on heritability are summarised in an editorial by Munroe and Tinker.4 The current study adds to this data by demonstrating that the genetic heritability of RHR is maintained, despite effects of environmental factors, such as patients age. They conclude: “A maintained heritability of RHR supports the continued search for genetic factors underlying RHR to provide further insights into understanding the key physiological mechanisms explaining variation in RHR.” As we put this data in the context of other studies suggesting that a lower RHR in men might be associated with an increased risk of atrial fibrillation, we clearly have more to learn about RHR as a predictor of cardiovascular outcomes.
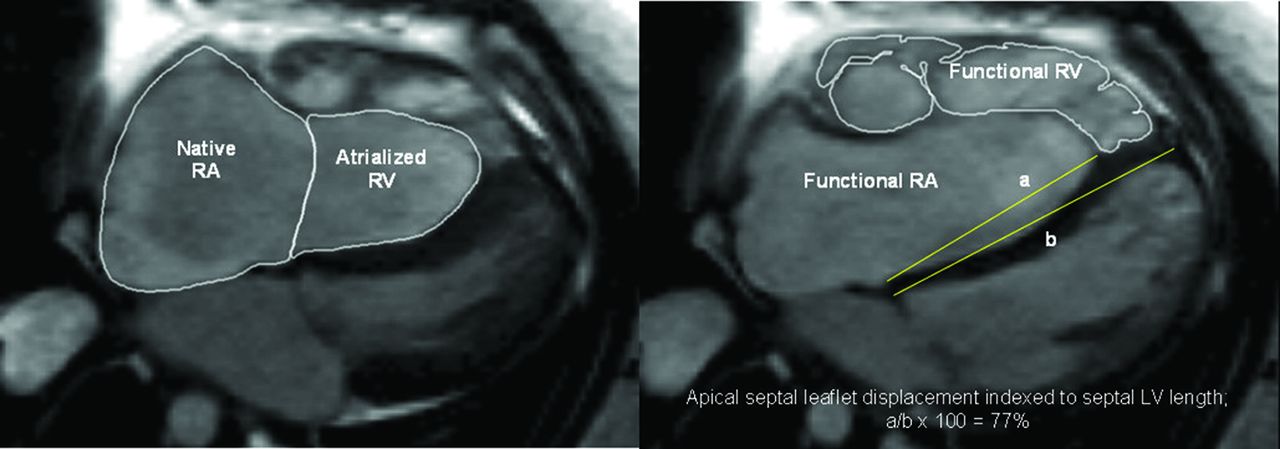
Advanced cardiac imaging has the potential to improve care of patients with complex cardiac disease. This is illustrated by a study of cardiac magnetic resonance (CMR) imaging in 79 adults with Ebstein’s anomaly of the tricuspid valve.5 CMR predictors of mortality (3.4 years follow-up) were right (RV) and left ventricular (LV) ejection fraction, LV stroke volume index and cardiac index (figure 2). Atrial tachycardia (AT) occurred in 22% and often preceded other adverse events. CMR predictors of AT were RV ejection fraction, the ratio of RV to LV volumes and the degree of apical displacement of the septal tricuspid valve leaflet (figure 3). This study demonstrates the value of CMR imaging to identify patients at risk adverse cardiac events, potentially justifying earlier intervention for structural disease. The importance of AT as a marker of increased risk also suggests that earlier or more aggressive arrhythmia prevention and management might be beneficial. The authors proposed composite of several CMR factors, in conjunction with other elements of shared decision making, is eminently reasonable.
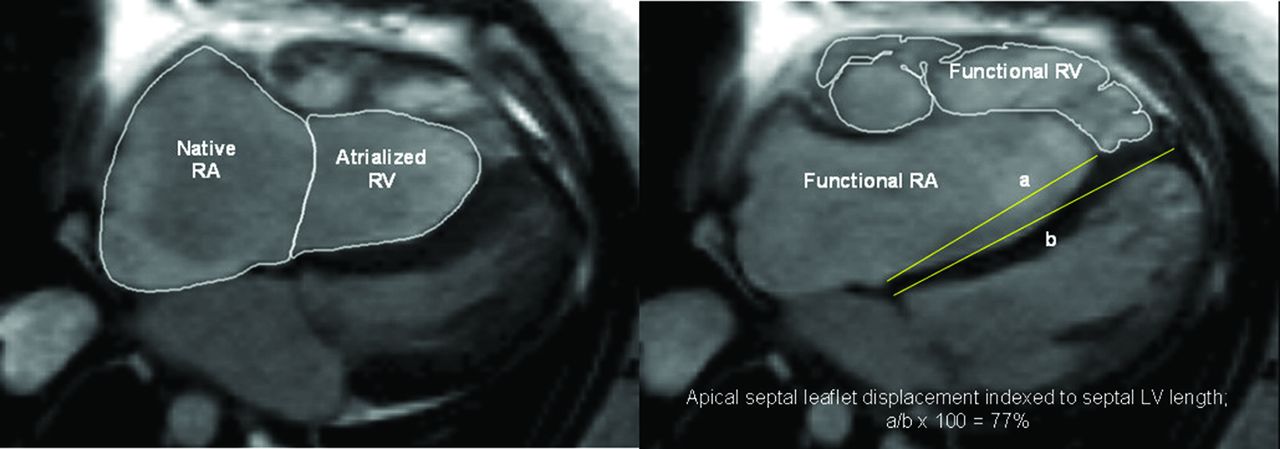
Measurements of native right atrial (RA) and atrialised right ventricular (RV) volumes, functional RV volumes and apical septal leaflet displacement/left ventricular (LV) septal length (A/B*100%). Steady-state free precession sequence and axial stack were used.

Survival curves for first-onset atrial tachycardia (n=65) stratified by univariable predictors with upper quartile functional right ventricular:left ventricular (LV) ratio (>2.4) and apical septal leaflet displacement/LV septal length (>67%) cut-offs accordingly.
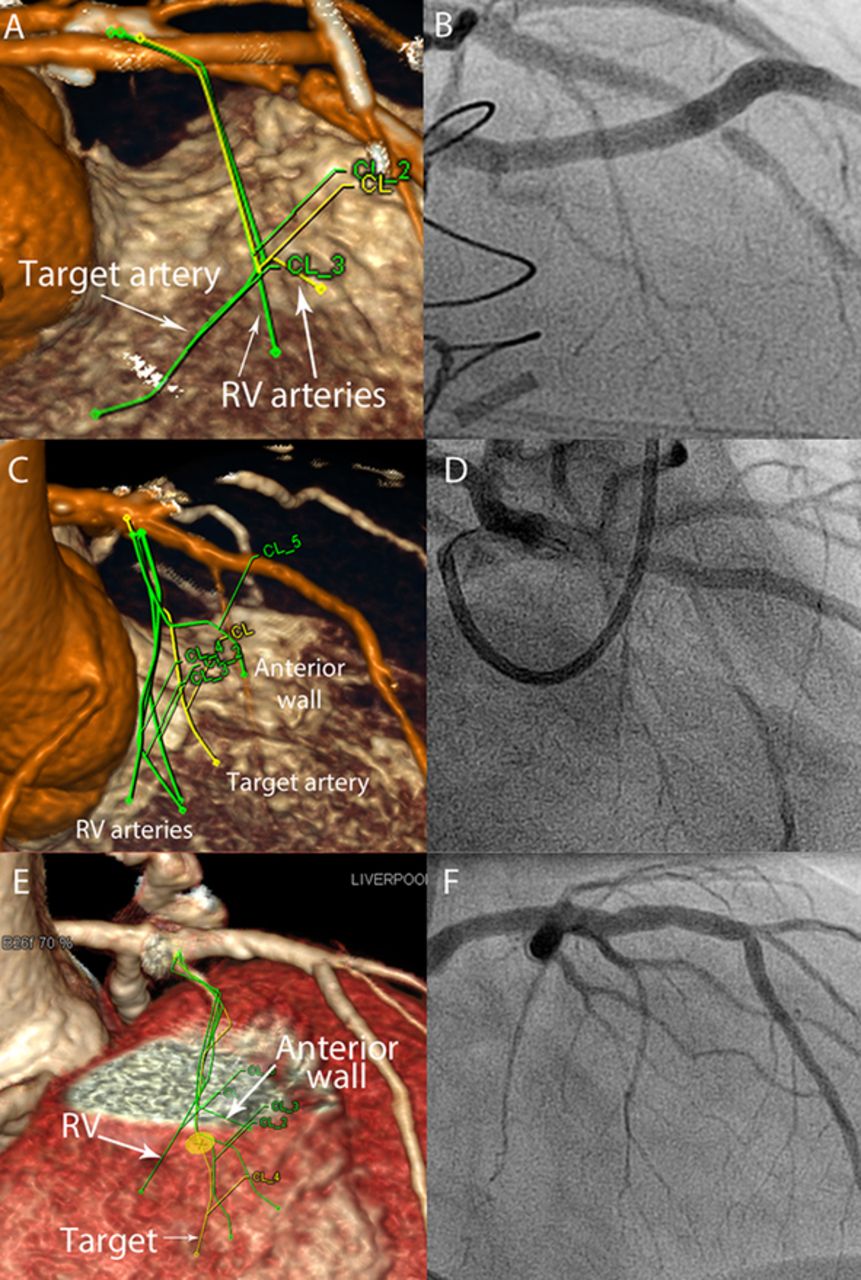
The Education in Heart article6 in this issue, discusses non-surgical septal reduction therapy for relief of subaortic outflow obstruction in adults with hypertrophic cardiomyopathy. This article includes indication, imaging approaches, technical aspects of the procedure itself and outcome data (figure 4).
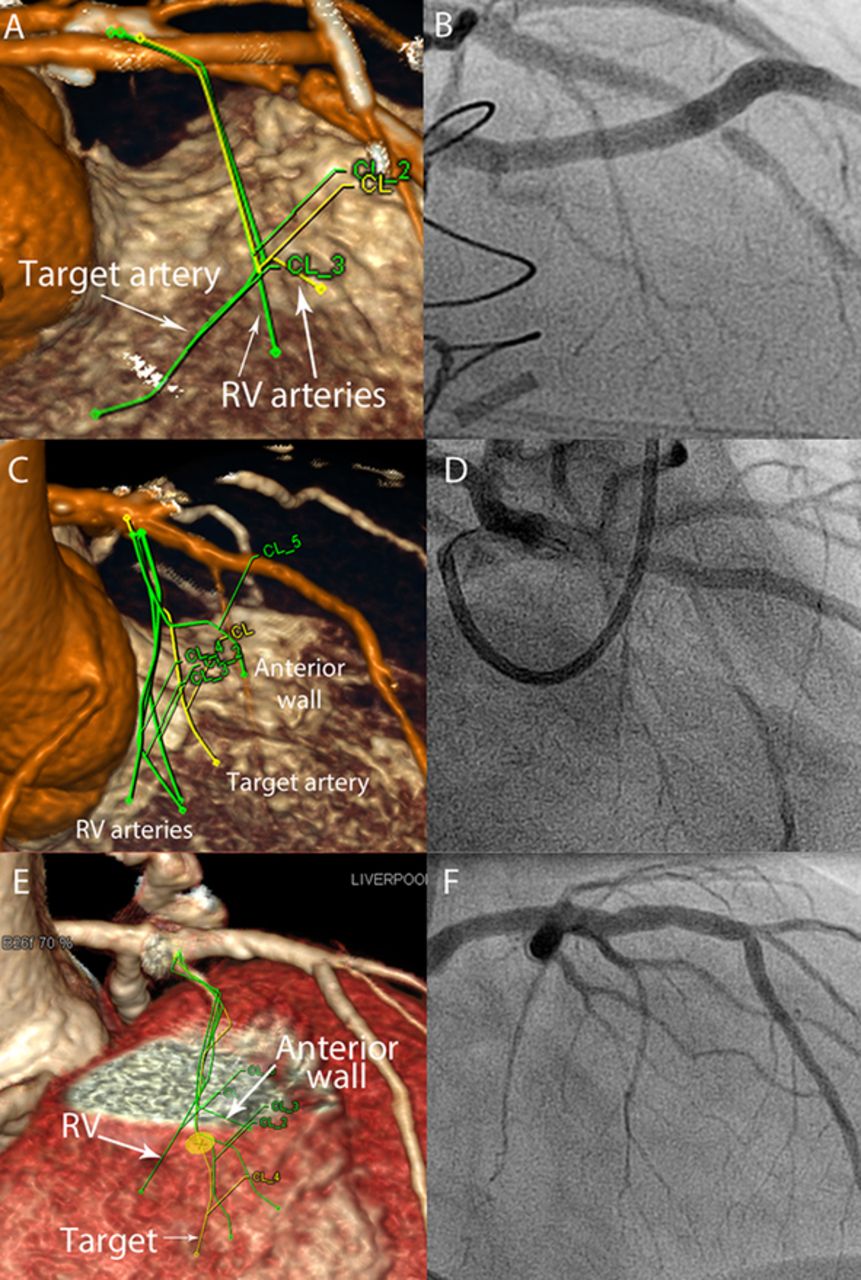
(A) CT angiogram. The traced septal vessels from two-dimensional images were projected on to the coronary angiogram ‘map’. This CT angiogram is rotated to minimise foreshortening and remove overlap (in this example to RAO cranial). The equivalent invasive angiogram projection is shown in (B). The target artery is identified and only this sub-branch is occluded for alcohol delivery. Further examples are shown in (C, D) and (E, F). RAO, right anterior oblique; RV, right ventricular.
A review article in this issue by Sannino and Grayburn7 on diagnosis and management of mitral regurgitation in adults with AS is not to be missed. The dilemma is whether to treat both AS and mitral regurgitation at the same time or whether to treat AS first to see if mitral regurgitation improves. In the interventional era, many patients have both valve lesions and the answer is not easy (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proposed algorithm for the evaluation and management of patients with severe aortic stenosis (AS) and concomitant mitral regurgitation (MR). ASE, American Society of Echocardiography; CMR, Cine Magnetic Resonance; CRT, cardiac resynchronization therapy; LV, left ventricular; MVR, mitral valve replacement; RHLC, right and left heart catheterisation; SAVR, surgical aortic valve replacement; TAVR, transcatheter aortic valve replacement; TEE, transoesophageal echocardiography.
Footnotes
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.