Article Text

Statistics from Altmetric.com
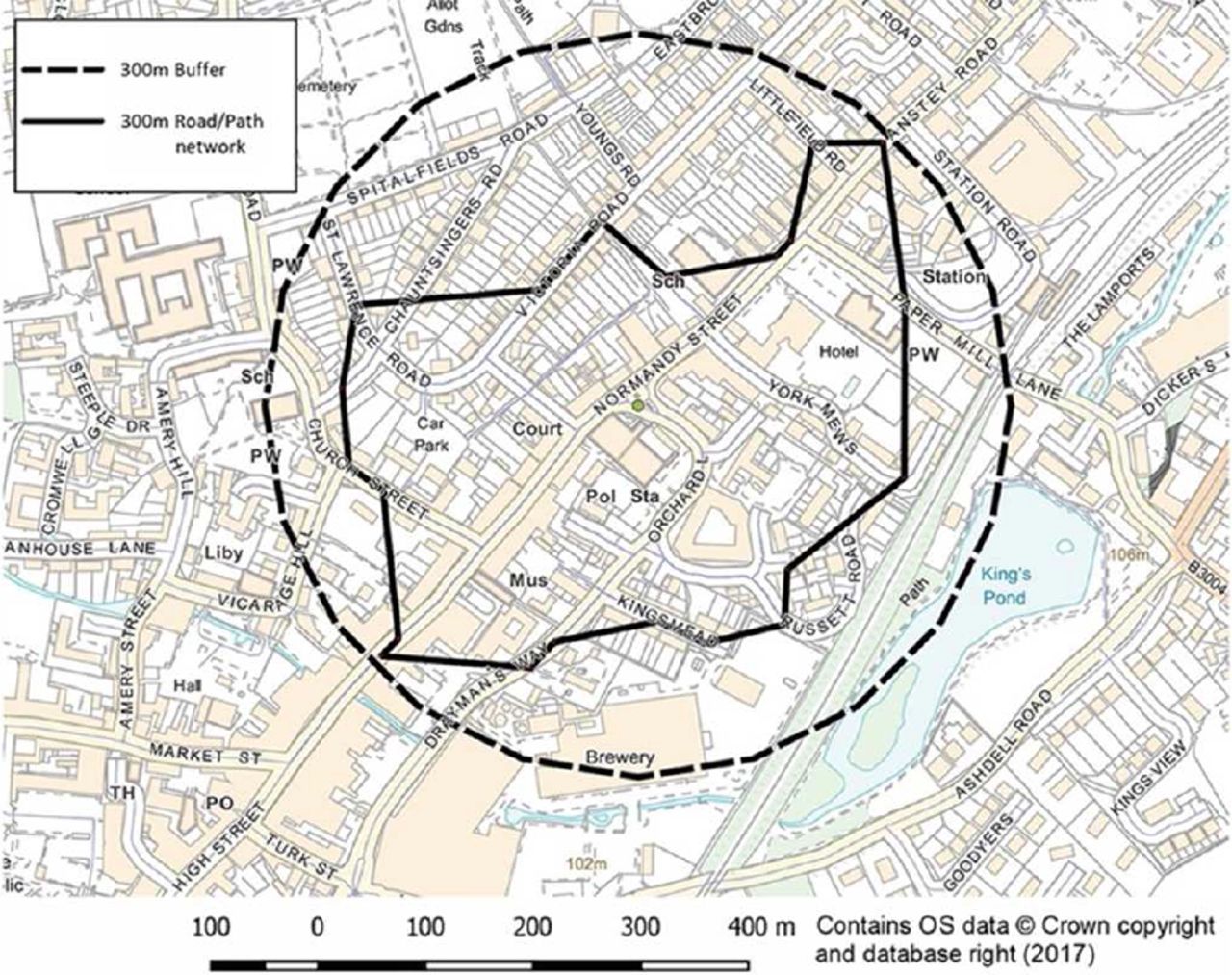
Out-of-hospital cardiac arrest (OHCA) is frequently the first manifestation of heart disease and early defibrillation, using a public access defibrillator (PAD) by bystanders, can improve the chance of survival and recovery. In this issue of Heart, Deakin et al 1 report a modelling study based on real-world data, using mapping software and realistic modelling assumptions, to compare suspected cardiac arrests identified by the dispatch centre with the geo-coordinates of the PAD registry for the South Central Ambulance Service region of England (figure 1). Their goal was to match the overall distribution of PADs in relation to OHCAs, both by actual walking distance and by retrieval times, as well as to evaluate the effects of reduced PAD availability at night and compare potential retrieval times with actual ambulance response times. From a total of 4130 calls to the dispatch centre used for data analysis in 2 years of study, they found that a PAD was available within 100 m of the event in almost 5.9% of OHCA during daytime hours, but this availability fell to less than 2% during overnight hours. As expected, distances to rural PADs were greater than in urban areas. The study determined that a PAD could be delivered to scene ahead of the ambulance arrival in in 25.3% of suspected OHCA. The authors recognise limitations of the study, many of them inherent to its modelling nature, and conclude that existing PADs are underused and there is currently considerable potential to improve bystander defibrillation rates by better usage of existing devices, particularly by ensuring they are all available on a 24-hours-a-day and 7-days-a-week basis.

Mapping representation showing the coverage achieved with a 300 m walking radius compared with the traditional coverage using a linear radius over the same distance.
In the companion editorial, Rea2 elegantly put the article in the context of the challenge of improving the effectiveness and the scope of public access defibrillation, commenting the potential role of new technologies, including social media and smart technologies. The take-home message is that we should think creatively about how to deliver a proven therapy to the right place at the right time, moving from a ‘public access’ approach to an ‘all-access’ defibrillation for most OHCA.
The use of PADs in sports centres is an area of special concern given that ‘sudden cardiac arrest is a rare but tragic event during amateur sports activities’. Based on prospectively collected data from 252 sports facilities over an 18-year period, Aschieri and colleagues3 were able to compare response times and survival rates at centres with and without an on-site PAD. Although the number of events was low (n=26, 92% men, mean age 54 years), neurologically intact survival was much higher for the 15 patients who arrested at centre with an on-site PAD compared with the 11 who arrested at centres without a PAD (93% vs 9%, p<0.001) (figure 2).

Temporal pattern of automated external defibrillation (AED) placed over the study period and its relationship with the probability that a sudden cardiac arrest (SCA) occurs in a centre with or without on-site AED. At the bottom of the figure, the outcomes of those SCAs that occurred in centres with an on-site AED are shown, whereas at the top of the figure the outcomes of those SCAs that occurred in centres without on-site AED are shown. Note the relationship between the rate of centres with on-site AED and the probability of neurologically intact survival.
The challenge of proving that PADs save lives in the absence of randomised controlled clinical trials is addressed in an editorial by Calle and Mpotos.4 Despite the apparent impressive difference in survival at centres with a PAD seen by Ascheiri et al,3 like any observational study, there are potential biases that may affect the results due to lack of randomisation, changes over time in awareness and treatment for OHCA, and other confounding factors. Even so, ‘from many studies, it is beyond any doubt that automated external defibrillation can be used properly by lay people and that this approach has the potential to save numerous lives’. Given that randomised trials of PADs are unlikely, ‘it should be stressed that all research should be based on data gathered in accordance with the internationally accepted Utstein definitions’.
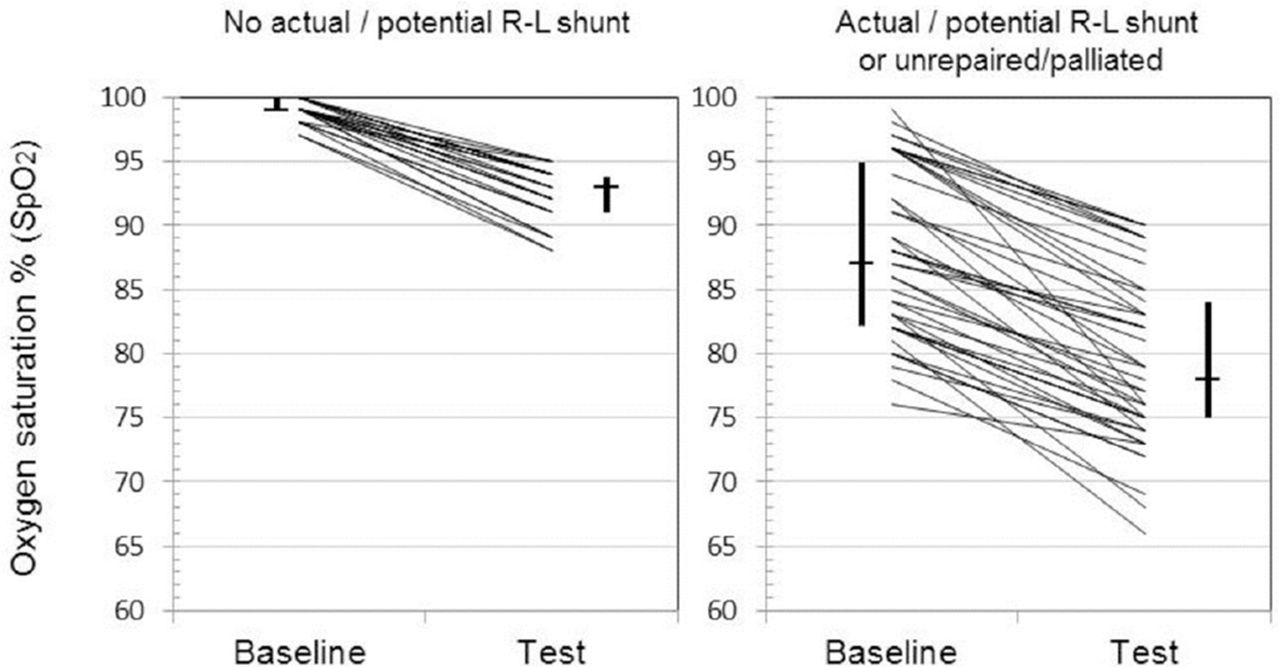
Many of us are aware that the air pressure in commercial airplanes is similar to being at 8000 feet (2438 m) elevation, with an equivalent cabin fraction of inspired oxygen of 0.15 (compared with 0.21 at sea level), leading to reduced oxygen saturation (SpO2) in passengers. While many of us might notice minor or no effects of the lower air pressure, our patients with heart disease might be more seriously affected. In order to identify which children with congenital heart disease might need supplemental in-flight oxygen, Naqvi and colleagues5 performed hypoxic challenge testing6 in 68 children (mean age of 3.3 years) with test failure defined by the degree of oxygen desaturation relative to baseline oxygen saturation levels. Children with no right to left shunt desaturated from a median of 99% to 93%, but none failed the challenge test. In contrast, children with an actual or potential right to left shunt desaturated from a median of 87% to 78% and 19% failed the test (figure 3).

{kind=link}
{kind=link}
{kind=link}
Baseline and hypoxic challenge testing SpO2 for those with no actual/potential R–L shunt (n=25) versus those with an actual/potential R–L shunt or unrepaired/palliated (n=43). Also shown are medians (horizontal line) and IQRs (vertical lines). R–L, right to left; SpO2, arterial oxygen saturation measured by pulse oximetry.
In an editorial, Files and Deen7 suggest caution is needed in routinely recommending hypoxic challenge testing in congenital heart patients “because it remains unknown if significant metabolic derangements arise in children with congenital heart disease in the setting of arterial desaturation. It is also unclear whether desaturation in itself is clinically worrisome. Simply put, desaturation does not equal tissue ischaemia, and a test failure may not necessarily translate into a clinical safety issue”. In addition, there are logistic issues in the availability and feasibility of hypoxic challenge testing, particularly in younger children, and in implementation of supplemental in-flight oxygen, particularly on long flights. Even so, ‘the primary finding of Naqvi’s report, that primarily children with an actual or potential right-to-left shunt are at risk for significant acute desaturation in the setting of hypoxia, is undoubtedly important’ and ‘provides much needed data to inform shared decision-making between congenital heart providers, their patients and their families’.
The Education in Heart article in this issue provides an overview of the evidence and guidelines relating to a multidisciplinary approach to heart failure.8 Although there is no standard definition of multidisciplinary care, interventions typically include education, self-monitoring and management; telemonitoring; structured telephone support; clinical review; medication management and cardiac rehabilitation. The elements summarised in this article will be helpful to centres starting a multidisciplinary heart failure programme and those seeking to improve an existing one.
Footnotes
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Commissioned; internally peer reviewed.