Article Text

Abstract
Objectives Differences in terms of safety and efficacy of percutaneous edge-to-edge mitral repair between patients with functional and degenerative mitral regurgitation (MR) are not well established. We performed a systematic review and meta-analysis to clarify these differences.
Methods PubMed, EMBASE, Google scholar database and international meeting abstracts were searched for all studies about MitraClip. Studies with <25 patients or where 1-year results were not delineated between MR aetiology were excluded. This study is registered with PROSPERO.
Results A total of nine studies investigating the mid-term outcome of percutaneous edge-to-edge repair in patients with functional versus degenerative MR were included in the meta-analysis (n=2615). At 1 year, there were not significant differences among groups in terms of patients with MR grade≤2 (719/1304 vs 295/504; 58% vs 54%; risk ratio (RR) 1.12; 95% CI: 0.86 to 1.47; p=0.40), while there was a significantly lower rate of mitral valve re-intervention in patients with functional MR compared with those with degenerative MR (77/1770 vs 80/818; 4% vs 10%; RR 0.60; 95% CI: 0.38 to 0.97; p=0.04). One-year mortality rate was 16% (408/2498) and similar among groups (RR 1.26; 95% CI: 0.90 to 1.77; p=0.18). Functional MR group showed significantly higher percentage of patients in New York Heart Association class III/IV (234/1480 vs 49/583; 16% vs 8%; p<0.01) and re-hospitalisation for heart failure (137/605 vs 31/220; 23% vs 14%; p=0.03). No differences were found in terms of single leaflet device attachment (25/969 vs 20/464; 3% vs 4%; p=0.81) and device embolisation (no events reported in both groups) at 1 year.
Conclusions This meta-analysis suggests that percutaneous edge-to-edge repair is likely to be an efficacious and safe option in patients with both functional and degenerative MR. Large, randomised studies are ongoing and awaited to fully assess the clinical impact of the procedure in these two different MR aetiologies.
- percutaneous edge-to-edge repair
- functional mitral regurgitation
- degenerative mitral regurgitation
- meta-analysis
Statistics from Altmetric.com
- percutaneous edge-to-edge repair
- functional mitral regurgitation
- degenerative mitral regurgitation
- meta-analysis
Introduction
Mitral regurgitation (MR) affects about 10% of people aged more than 75 years and is the second most common valve disease requiring surgery in Europe.1 Surgical mitral valve (MV) intervention is currently considered the gold standard for treatment of symptomatic patients with severe degenerative MR (DMR).1 2 The role of surgery for functional MR (FMR) is less well defined. Nevertheless, a significant number of patients with symptomatic MR have extensive comorbidities or uncertain indications for surgery and are defined as high surgical risk, inoperable or not indicated for surgery, and approximately one-half of patients with symptomatic severe MR may not undergo surgery.3 The edge-to-edge percutaneous mitral repair performed with the MitraClip device (Abbott Vascular, Menlo Park, California, USA) was reported to be safe and effective, even in high-risk patients,4 5 and it is the most widely catheter-based strategy used to treat MR. According to American Heart Association/American College of Cardiology guidelines, percutaneous edge-to-edge repair is currently recommended only for patients with DMR who have severe symptoms and are at high or prohibitive risk of surgery (recommendation class IIb, level of evidence B),2 while European Society of Cardiology/European Association for Cardio-Thoracic Surgery guidelines approved it for both DMR and FMR (recommendation class IIb, level of evidence C).1 Between DMR (or primary) and FMR (or secondary), there are important differences in terms of MV morphology, clinical characteristics (ie, age, comorbidities), left ventricular (LV) function, therapies and clinical outcomes. In case of degenerative aetiology, MR is due to MV apparatus intrinsic lesions. Recovery of mitral competence with mitral repair abolishes the haemodynamic burden responsible for the deterioration in LV function, may restore it if already depressed, and improves both quality of life and long-term outcome.6
In FMR, treating MR does not cure the ischaemic myocardial dysfunction or dilated cardiomyopathy that caused the regurgitation in the first place. Thus, restoration of mitral competence in this setting does not correct the underlying cause of MR, and this may not lead to improvement in LV function. Moreover, it does not definitely improve longevity, although it improves quality of life.7 Therefore, our aim was to systematically review the published literature about percutaneous edge-to-edge repair outcome and perform a meta-analysis of studies investigating the differences after percutaneous edge-to-edge repair in these two very different aetiologies for which it is being applied.
Methods
Search strategy and study selection
In this study, the search strategy, study selection, data extraction and data analysis were performed in accordance with The Cochrane Collaboration and the Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines.8 Meta-Analyses and Systematic Reviews of Observational Studies (MOOSE) checklist has been followed.9
All randomised controlled trials (RCTs) and observational studies reporting 1-year outcome after MitraClip procedure and delineated between the aetiology of MR (last update 11 January 2016) were evaluated for inclusion in the meta-analysis. We excluded studies with less than 25 patients, or with overlapping populations. Two authors (MC, CG) independently searched PubMed, Embase, BioMedCentral, Google Scholar and the Cochrane Central Register of Controlled Trials. In addition, we employed backward snowballing (ie, review of references from identified articles and pertinent reviews) and searched abstracts from 2014 and 2016 relevant scientific meetings (Transcatheter Cardiovascular Therapeutics, AHA, ACC, ESC, EuroPCR and PCR London Valves). The search strategy for PubMed is available as online supplementary material. This study is registered with PROSPERO number CRD42016048042.
Data extraction
Two investigators (MC, CG) independently assessed studies for possible inclusion. Non-relevant articles were excluded based on title and abstract. Two authors (MC, AS) independently extracted data on study design, measurements, patient characteristics and outcomes. Data extraction conflicts were discussed and resolved with another author (MP). Missing data were requested by means of email to the corresponding author of each study. In the case of studies with overlapping populations, only the manuscript reporting the largest number of patients was selected.
Outcomes
Primary efficacy endpoints were the percentage of patients with MR grade ≤2 and the rate of MV re-intervention (surgical and/or percutaneous) at 1 year. Secondary efficacy endpoints were the 1-year rate of overall mortality, and percentage of patients in New York Heart Association (NYHA) class III/IV.
Primary safety endpoints were 1-year rate of single leaflet device attachment (SLDA) and device embolisation.
Every endpoint was assessed according to the definitions reported in the original study protocols.
All analyses were performed according to the intention-to-treat (ITT) principle. Whenever it was possible, we performed the analyses also considering the as-treated with follow-up population, in order to assess consistency among ITT and as-treated with follow-up analyses.
Statistical analysis
Continuous variables were reported as mean and SD. We compared the pooled baseline characteristics of both groups, presenting continuous variables as pooled weighted means and composite SD. When baseline data were available only as median and IQR, mean and SD were calculated.10
Pooled risk ratios (RRs) for categorical variables (dichotomous outcomes) were calculated using a binary random effects model, with the Mantel-Haenszel method.11 In studies in which no events were reported within groups, the difference between aetiology groups could not be assessed. The hypothesis of statistical heterogeneity was tested by means of Cochran Q statistic and I2 values. I² values of <40%, 40%–60% or >60% indicated low, moderate or substantial heterogeneity, respectively.12 Statistical tests of publication bias were not used to detect funnel-plot asymmetry because <10 studies were included in this study. Therefore, we visually estimated funnel plots to evaluate the possibility of publication bias.13
Sensitivity and subgroup analyses were performed to assess the extent of which several covariates might have affected the risk estimates for the outcomes.
Computation was performed with RevMan (Review Manager V.5.3, The Nordic Cochrane Center, The Cochrane Collaboration, Copenaghen, 2014) and Stata (V.13.1, Stata).
Results
Study selection
A total of seven published articles5 14–19 and two studies presented at the EuroPCR 2014 and 2015 conferences20 21 were included in the meta-analysis. One study was a RCT,20 while the remaining eight studies were prospective observational registries. Figure 1 shows the flow chart of the study selection process.

Flow chart of the study selection process. ACC, American College of Cardiology; AHA, American Heart Association; ESC, European Society of Cardiology; MR, mitral regurgitation; TCT, Transcatheter Cardiovascular Therapeutics.
Characteristics of the included studies
Two studies included patients with mixed MR aetiologies17 18: we excluded from the analyses 90 patients with both DMR and FMR aetiologies, in order to reduce confounding results. The main features of the included studies are summarised in table 1. A total of 2615 patients undergoing percutaneous edge-to-edge repair were analysed: 1782 patients presented with FMR and 833 patients with DMR. For 1481 out of 2615 patients, preprocedural echocardiographic assessment data regarding LVEF and left ventricular end diastolic volume (LVEDV) were reported in the included studies.
Main features of the studies included in the meta-analysis
Baseline patients’ features
Baseline clinical and echocardiographic features are shown in tables 2 and 3. Patients in the FMR group presented more comorbidities and the higher risk profile, while patients with DMR were significantly older (73±9.68 vs 78±10.55 years, p<0.001). No differences were found in terms of atrial fibrillation (54% vs 56%, FMR vs DMR, respectively, p=0.214). LVEDV and left ventricular end diastolic diameter (LVEDD) were both significantly higher in patients with FMR; in addition, LVEF was significantly lower in patients with FMR compared with those affected by DMR (38.5%±13% vs 58.3%±10.4%, p<0.001). There was also a significantly higher percentage of patients with FMR in NYHA class≥3 at baseline (86.6% vs 75.6%, p<0.001). MR grade≥3 at baseline was present in 2088 out of 2295 patients (91%), with a significantly lower percentage in patients with FMR (88.9% vs 95.2%, p<0.001).
Baseline clinical features in the studies included in the meta-analysis
Baseline NYHA class and echocardiographic features in the studies included in the meta-analysis
Acute procedural success was achieved in 95% of patients, without differences between groups (95% vs 94%, FMR vs DMR, respectively, p=0.52) (online supplementary figure S1).
One-year outcome
MR grade at 1-year follow-up was reported in six out of nine studies, without significant differences in terms of percentage of patients with MR grade≤2 (RR 0.91; 95% CI: 0.76 to 1.09; p=0.30), with evidence of substantial heterogeneity among studies (I2 =80%) (figure 2).

Risk estimates of MR grade≤2 for functional MR versus degenerative MR. Forest plot shows results for MR grade≤2 at 1 year. EVEREST II, Endovascular Valve Edge-to-Edge Repair Study II; HRR, High Risk Registry; MR, mitral regurgitation.
MV re-intervention at 1 year was reported in eight out of nine studies, and there was a significantly lower rate in patients with FMR compared with those with DMR (4% vs 10%, FMR vs DMR, respectively; RR 0.60; 95% CI: 0.38 to 0.97; p=0.04), with low heterogeneity among studies (I2 =33%) (figure 3).

Risk estimates of MV re-intervention for functional mitral regurgitation versus degenerative mitral regurgitation. Forest plot shows results for MV re-intervention at 1 year. EVEREST II, Endovascular Valve Edge-to-Edge Repair Study II; MV, mitral valve.
As shown in figures 4, 1-year rate of overall mortality (reported in eight studies) was not significantly different between groups (18% vs 14%, FMR vs DMR, respectively; RR 1.26; 95% CI: 0.90 to 1.77; p=0.18), with moderate heterogeneity between studies (I2 =55%).

Risk estimates of overall mortality for functional mitral regurgitation versus degenerative mitral regurgitation. Forest plot shows results for overall mortality at 1 year. EVEREST II, Endovascular Valve Edge-to-Edge Repair Study II; RCT, randomised controlled trial.
In contrast, FMR aetiology was associated with a higher percentage of patients in NYHA class III/IV at 1 year (14% vs 7%, FMR vs DMR, respectively; RR 1.75; 95% CI: 1.31 to 2.36; p<0.001), without evidence of statistical heterogeneity among studies (I2 =0%) (online supplementary figure S2). A significantly higher rate of re-hospitalisation for heart failure was reported in patients with FMR (RR 1.74; 95% CI: 1.05 to 2.85; p=0.03), with moderate heterogeneity among studies (I2 =46%) (online supplementary figure S3).
All primary and secondary efficacy endpoints estimates were consistent with those assessed in the as-treated analysis (see online supplementary figures S4-S8), except for non-significant differences in term of MV re-intervention (4% vs 12%, FMR vs DMR, respectively; RR 0.61; 95% CI: 0.37 to 1.01; p=0.06) and of re-hospitalisation for heart failure, and a lower grade of heterogeneity in comparison to the ITT analysis.
{kind=link}
![[SP1.png]](https://heart.bmj.com/content/heartjnl/104/4/306/DC1/embed/inline-supplementary-material-1.png?download=true){kind=link}
{kind=link}
{kind=link}
{kind=link}
![[SP2.png]](https://heart.bmj.com/content/heartjnl/104/4/306/DC2/embed/inline-supplementary-material-2.png?download=true){kind=link}
![[SP3.png]](https://heart.bmj.com/content/heartjnl/104/4/306/DC3/embed/inline-supplementary-material-3.png?download=true){kind=link}
{kind=link}
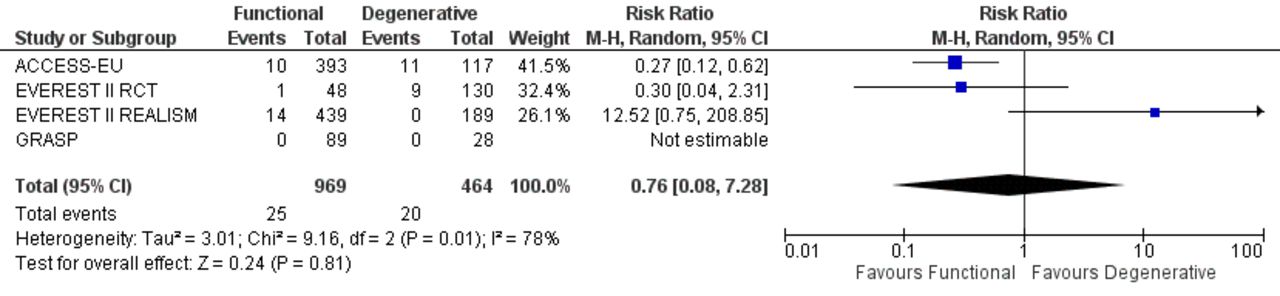
Risk estimates of primary safety endpoints for functional mitral regurgitation versus degenerative mitral regurgitation. Forest plot shows results for single leaflet device attachment at 1 year. Results of device embolisation are not shown because no events were reported among studies. EVEREST II, Endovascular Valve Edge-to-Edge Repair Study II; RCT, randomised controlled trial.
Primary safety endpoints at 1 year were reported in four out of nine studies. No events of device embolisation were reported among studies, while single leaflet device attachment was reported only in 45 out of 1433 patients (3%), without differences between patients with FMR and DMR (RR 0.76; 95% CI: 0.08 to 7.28; p=0.81), and with evidence of substantial heterogeneity among studies (I2 =78%) (figure 5).
Furthermore, we derived funnel-plot distributions of primary efficacy endpoints from the SE of the logRR plotted against the logRR confirming the absence of publication bias and small study effect for MV re-intervention, while there were evidence for the presence of small-study effects for MR grade≤2 (online supplementary figures S9 and S10).
Finally, the percentage of patients with MR grade≤2 was consistent at sensitivity analyses performed including only studies with the explicit inclusion criterion of MR grade≥3 at baseline (RR 1.02; 95% CI: 0.91 to 1.14; p=0.74).5 16 17 21
Discussion
To the best of our knowledge, this is the first meta-analysis of prospective studies investigating the differences, in terms of 1-year efficacy and safety, between FMR and DMR after percutaneous edge-to-edge mitral repair. The main findings for the two aetiology groups are as follows:
Percentages of patients with MR grade≤2 at 1 year were similar between FMR and DMR groups.
Patients with FMR had a significantly lower 1-year rate of MV re-intervention compared with DMR.
Similar rate of 1-year overall mortality was reported between FMR and DMR groups.
No differences were found in terms of 1-year single leaflet device attachment and device embolisation rates.
Conversely, a significantly higher percentage of patients in NYHA functional class III/IV and a higher rate of re-hospitalisation for heart failure were reported in patients with FMR.
FMR and DMR are two conditions that differ each other in several ways. Unfortunately, only the Endovascular Valve Edge-to-Edge Repair Study II RCT has investigated acute, mid and long-term outcome after the percutaneous edge-to-edge repair, and with more than 2/3 of patients with DMR it was not powered enough to assess any eventual difference due to MR aetiology.4
To fully understand the role of percutaneous MV repair, we evaluated the major differences reported in the present meta-analysis, which pooled the results of all RCT and observational studies reporting 1-year outcome after percutaneous edge-to-edge repair according to MR aetiology.5 14–21 As expected, baseline features of patients affected by FMR resulted in significantly higher cardiovascular risk profile compared with patients with DMR. In addition, the echocardiographic features reported that patients with FMR were characterised by significantly lower LVEF and higher LVEDD and LVEDV, in agreement with underlying pathophysiological mechanisms of the two aetiologies.22
The presence of low LVEF due to negative LV remodelling makes the potential benefits of percutaneous edge-to-edge repair less predictable in terms of clinical and echocardiographic outcomes in patients with FMR.23 24 Therefore, it is important to remark the high percentage of patients with MR grade≤2 reported at 1 year in our study in both groups (85% in the as-treated with follow-up population) without significant differences between groups. MR recurrence is frequent after surgical MV repair in patients with FMR, with 14%–66% of patients with MR grade>2 at follow-up23 25 26; conversely, surgical MV repair has shown durable results in patients with DMR, with a risk of recurrence of moderate-to-severe MR of 1%–2% only per year.27 Thus, our results emphasise the positive impact that the percutaneous edge-to-edge repair can achieve in case of FMR.28 Indeed, the absence of severe MR recurrence, a main concern expected in FMR because of the progressive LV dysfunction,23 could be considered a sign of interruption of the LV dilation-MR worsening loop.24 Animal data demonstrate that reduction in MR severity to a regurgitant fraction of approximately one-third (moderate MR) allows for reverse remodelling and improved muscle function in case of LV dysfunction.29 Reverse LV remodelling after percutaneous edge-to-edge repair was reported mostly in patients with no advanced heart failure (LVEF>30%) and without severe LV dilation (LVEDD<70 mm, LVEDV<200 mL)28; reverse LV remodelling is unlikely also after MV surgery in case of FMR with dilated and compromised LV at baseline.23 Conversely, maintaining of optimal results at follow-up is more achievable after successful procedure in patients with DMR, because of less frequent LV dysfunction.30
After surgical MV repair, MV re-intervention rates reported in literature range between 3% and 5%, and are similarly low in both FMR26 and DMR.31 Therefore, an unexpected finding of our study was the significantly lower rate of MV re-intervention reported in patients with FMR (4%) compared with those with DMR (10%), despite a comparable rate of SLDA among groups (3% vs 4%, FMR vs DMR, respectively, p=0.81), leading us to look for further explanation. It is reasonable to speculate that baseline surgical risk profile (higher in patients with FMR) could have limited the decision of surgical re-intervention during follow-up, even when these patients had deteriorated, especially in those needing cardiac surgery. Indeed, in a subanalysis on patients with FMR from the ACCESS-Europe A Two-Phase Observational Study of the MitraClip System in Europe (ACCESS-EU) registry, most of the MV re-interventions performed at follow-up were reported in patients with LVEF>40%.32 Similar results were observed considering other important risk factors, such as chronic kidney disease, which was less frequent in those who underwent surgical re-interventions.33
Our results showed comparable overall mortality rate between groups (18% vs 14%, FMR vs DMR, respectively, without substantial heterogeneity among studies), despite the higher risk profile characterising patients with FMR, which predisposes to worse outcome in these patients compared with those with DMR,3 also after surgical MV repair.34 In fact, the overall mortality rate after surgical repair of FMR ranges from 20% to 50%.7 25 Conversely, long-term survival after surgical repair of DMR is similar to that observed in the age-matched general population.35 Thus, looking at data of this meta-analysis, it seems that the percutaneous edge-to-edge repair was selected for patients with FMR due to the less clear indications for surgery, compared with DMR where comorbidities influenced the choice for percutaneous edge-to-edge repair rather than surgery. We have to take into account that the more advanced age reported in patients with DMR could have counterbalanced the effects of other important risk factors and comorbidities present in patients with FMR. However, the high overall mortality rate reported in our meta-analysis (16%) seems to reflect the excessively high-risk profile of treated patients, which is near to those reported by Goel et al in inoperable patients with MR (90% with FMR) treated with medical therapy alone (20% at 1 year and 50% at 5 years).3 In the future, it could be that better patient selection and performing percutaneous edge-to-edge repair at earlier stage could avoid treatment of those patients with advanced LV remodelling, more than severe MR, and many comorbidities, who benefit less from the procedure. The reassuring safety features (only 3% of 1-year rate of SLDA, and no events of device embolisation reported in our analysis) and the good efficacy profile of percutaneous edge-to-edge repair support the proposal to consider this treatment as a primary tool for patients with FMR and not only as a rescue therapy.
Ongoing trials, such as the A Multicenter, Randomised, Controlled Study to Assess Mitral vAlve reconsTrucTion for advancEd Insufficiency of Functional or iscHemic ORigiN (MATTERHORN, NCT02371512) RCTs, in which the percutaneous edge-to-edge repair is compared with surgical repair or replacement in patients with FMR, and the Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients With Functional Mitral Regurgitation (COAPT, NCT01626079), and the Multicentre Study of Percutaneous Mitral Valve Repair MitraClip Device in Patients With Severe Secondary Mitral Regurgitation (MITRA-FR, NCT01920698) randomised trials, in which the percutaneous edge-to-edge repair is compared with optimal medical therapy in patients affected by FMR, should help to clarify the therapeutic position of percutaneous edge-to-edge repair in these setting of patients.
Study limitations
This article represents a study-level meta-analysis; therefore, a relevant limitation is the lack of patient-level data. In addition, the studies included in the analysis enrolled heterogeneous populations, and this is likely to have contributed significantly to the heterogeneity observed. Moreover, there were many differences between the two groups in terms of baseline features and comorbidities, due to fundamentally different nature of the DMR and FMR populations. As with any meta-analysis, our study shares possible limitations of the included studies. More in detail, only one out of nine studies had a randomised design. Finally, we were not able to assess the impact of acute procedural success and of postprocedural MR grade on clinical and echocardiographic outcome, because the included studies did not report these data stratified by MR aetiology.
Conclusions
Our meta-analysis suggests that percutaneous edge-to-edge repair appears to be a reasonable option in patients affected by both FMR and DMR, keeping into account the various therapeutic goals achievable in these two deeply different conditions. Large, randomised studies with extended follow-up are ongoing and awaited to fully assess the clinical impact of the percutaneous edge-to-edge repair in these two very different MR aetiologies.
Key messages
What is already known on this subject?
The percutaneous edge-to-edge repair has shown to be a good option for high-risk patients with mitral regurgitation (MR), even with end-stage systolic heart failure, but there is still no consensus on its use in patients with functional MR (FMR) because of the lack of randomised studies focusing on patients affected by FMR not amenable to surgery.
What might this study add?
In a meta-analysis of randomised and observational studies of patients affected by functional or degenerative MR (DMR) undergoing percutaneous edge-to-edge repair procedure, patients with FMR reported a lower rate of re-intervention than those with DMR (4% vs 10%; p=0.04) and a comparable rate of MR recurrence (58% vs 54%; p=0.40) and of mortality (18% vs 14%; p=0.18) after 1-year follow-up, despite a worse baseline risk profile.
How might this impact on clinical practice?
The extremely reassuring safety profile and the good efficacy shown in this meta-analysis support the proposal to definitively assess if this treatment could be considered a primary tool for patients with FMR and not only as a rescue therapy. Large ongoing randomised trials are hugely awaited to conclusively address this issue.
![[SP4.png]](https://heart.bmj.com/content/heartjnl/104/4/306/DC4/embed/inline-supplementary-material-4.png?download=true){kind=link}
![[SP5.png]](https://heart.bmj.com/content/heartjnl/104/4/306/DC5/embed/inline-supplementary-material-5.png?download=true){kind=link}
![[SP6.png]](https://heart.bmj.com/content/heartjnl/104/4/306/DC6/embed/inline-supplementary-material-6.png?download=true){kind=link}
![[SP7.png]](https://heart.bmj.com/content/heartjnl/104/4/306/DC7/embed/inline-supplementary-material-7.png?download=true){kind=link}
![[SP8.png]](https://heart.bmj.com/content/heartjnl/104/4/306/DC8/embed/inline-supplementary-material-8.png?download=true){kind=link}
![[SP9.png]](https://heart.bmj.com/content/heartjnl/104/4/306/DC9/embed/inline-supplementary-material-9.png?download=true){kind=link}
![[SP10.png]](https://heart.bmj.com/content/heartjnl/104/4/306/DC10/embed/inline-supplementary-material-10.png?download=true){kind=link}
References
Footnotes
Contributors Study conception and design: MC, CG, MP. Acquisition of data: MC, MP, EAM, MP, AS. Analysis and interpretation of data: MC, MP, EAM, GB-Z, GL, TF, OA, CG. Drafting of manuscript: MC, CG. Critical revision: GB-Z, AL, GL, MP, CDM, AM, FM, TF, OA, AC, CG.
Competing interests FM has received consulting fees from Abbott Vascular, Medtronic, ValtechCardio, and St. Jude Medical; is a founder of 4Tech; and has received royalties from Edwards Lifesciences. TF has received consulting fees and research support from Abbott, Boston Scientific, Edwards and WL Gore. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice Since this paper was first published online, the study variables in the top row of table 2 have been reformatted. They are now appearing above the correct columns.