Article Text

Abstract
Introduction Natriuretic peptides, including NTproBNP, are elevated in heart failure (HF) and correlate with prognosis. They also predict the development of HF and are associated with an adverse outcome in patients without overt HF. NICE CG108 mandates that patients with potential HF and elevated natriuretic peptides are evaluated with echocardiography and specialist assessment. There are few data on how outcomes compare based on whether the final diagnosis is HF or not after assessment. Furthermore, the incidence of subsequent HF in patients where the diagnosis is initially rejected is unknown.
Methods All patients with possible HF and raised NTproBNP referred to a single centre specialist HF clinic in a 1 year period from March 2014 were identified. Patients were seen within 2 (NTproBNP >2000 pg/ml) or 6 (NTproBNP 4002000 pg/ml) weeks of referral in line with NICE CG108. Hospital coding data and electronic patient records were used to identify all-cause unplanned hospital admissions and mortality over a minimum follow up period of 2 years. Event rates were compared between patients with a final diagnosis of HF and those without (no heart failure-NHF). We also recorded how many NHF patients went on to develop HF.
Results 235 patients were seen and form the study population. Mean follow up was 29±4 months. 133 (56%) patients were diagnosed with HF; 63 (47%) with HF with Reduced Ejection Fraction (HFREF) and 70 (53%) with HF with Preserved Ejection Fraction (HFPEF). 102 (43%) were diagnosed as NHF. Comorbidities in the NHF group are shown in table 2.
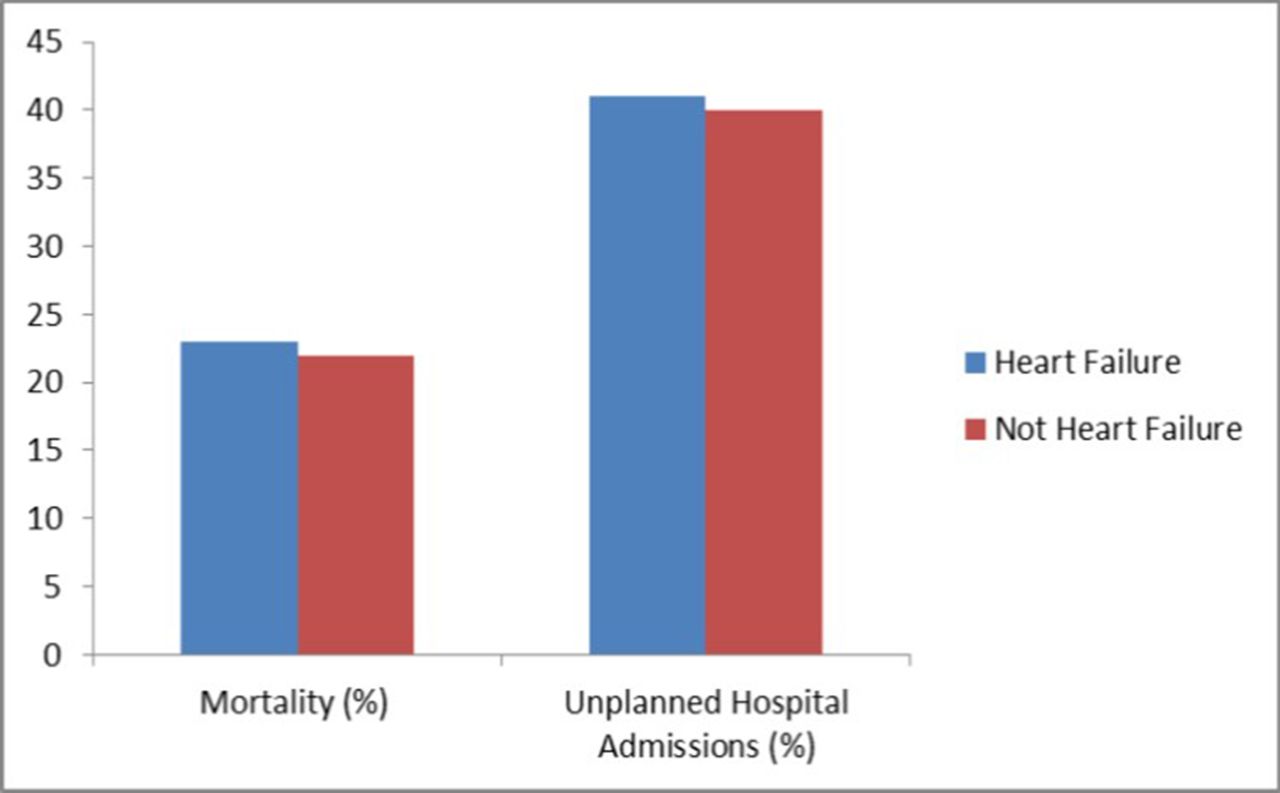
Patients in the two groups were similar in age. HF patients had much higher NTproBNP levels and higher rates of AF and diabetes (table 1). Despite this, there were no differences in either mortality (HF 23% and NHF 22%; p=0.75) or hospitalisations (HF 41% and NHF 40%; p=0.95) between the groups; figure 1.
Abstract 41 Table 1 Baseline characteristics of patients
Abstract 41 Table 2 Diagnoses of NHF group made at HF clinic assessment. Many patients had multiple diagnoses causing their symptoms and raised NTproBNP
7 (7%) of NHF patients were subsequently diagnosed with HF. Negative predictive value of a NHF diagnosis was 93%.
Conclusions Patients with suspected HF and raised natriuretic peptides are at high risk of adverse outcomes regardless of the final diagnosis after specialist evaluation. Much higher NTproBNP levels and higher rates of diabetes and AF in the HF group did not translate into a worse prognosis. This may be due to the fact that patients with a HF (in particular HFREF) diagnosis were considered for evidence based therapies. The adverse outcome in the NHF group is not explained by unrecognised HF at assessment as subsequent presentations with HF were uncommon. These findings should be taken into consideration when framing our discussions with all patients with elevated NTproBNP regarding their prognosis.

{kind=link}
Abstract 41 Figure 1 Mortality and unplanned hospitalisation rates between HF and NHF groups