Article Text

Abstract
Introduction Functional analysis of coronary artery stenosis is an important tool in the assessment of angiographic intermediate lesions. The deferral of treatment with percutaneous coronary intervention (PCI) of angiographic intermediate but functionally insignificant lesions has been shown to be non-inferior to optimal medical management. Deferral of PCI of a functionally non-significant stenosis is associated with a favourable very long-term follow-up without signs of late ‘catch-up’ phenomenon at 15 years. However assessment with FFR and selection of appropriate patients for intervention has been shown to improve outcomes in large studies demonstrating patients with stable CAD and FFR≤0.80, PCI reduces the composite rate of death, nonfatal MI, and urgent revascularization, compared to OMT alone, driven primarily by a reduction in urgent revascularization. FFR is generally safe and effective, however it must be measured during maximum hyperemia induced by a vasodilator such as adenosine. This has cost and time implications, and can be unpleasant for patients. Recently a novel tool in the assessment of intermediate lesions has become available in the form of instantaneous free wave ratio (iFR). This measures the difference between pressure distal to the coronary stenosis and aortic pressure (Pd/Pa) in the diastolic wave free period of the cardiac cycle where there is a linear relationship between pressure and flow. In large randomised control studies iFR has proven non inferior to FFR with respect to the risk of major adverse cardiac events at 1 year in both patients with stable angina and ACS The rate of adverse procedural effects was lower and the procedural time was shorter with iFR than with FFR leading to a modest cost benefit and a reduction in patient discomfort. Despite this, when assessing this new tool in our cath lab, we noticed some discordance between results, when iFR suggested treating or deferring and this was not corroborated by FFR. This discordance can have far reaching consequences for the patient and deserves careful consideration with a clear plan to uniformly approach such patients. One such option is to use a hybrid approach of iFR and FFR in patients with borderline measurements which has shown favourable results in similar studies.2 The level of discordance seen in our lab was similar to other large studies at 22.5%.6 7 Interestingly the large randomised control trials of iFR mentioned previously suggested that using iFR alone may also be a reasonable option.
Methods A total of 40 patients who had intermediate grade coronary stenosis visually were studied with both iFR and FFR measurements. The results were then compared in a hybrid fashion and revascularization strategy based on clinical picture and iFR and FFR measurements. The correlation between iFR and FFR was examined and the results graphed (figure 1). The cost benefit of not using adenosine was also considered.
{kind=link}
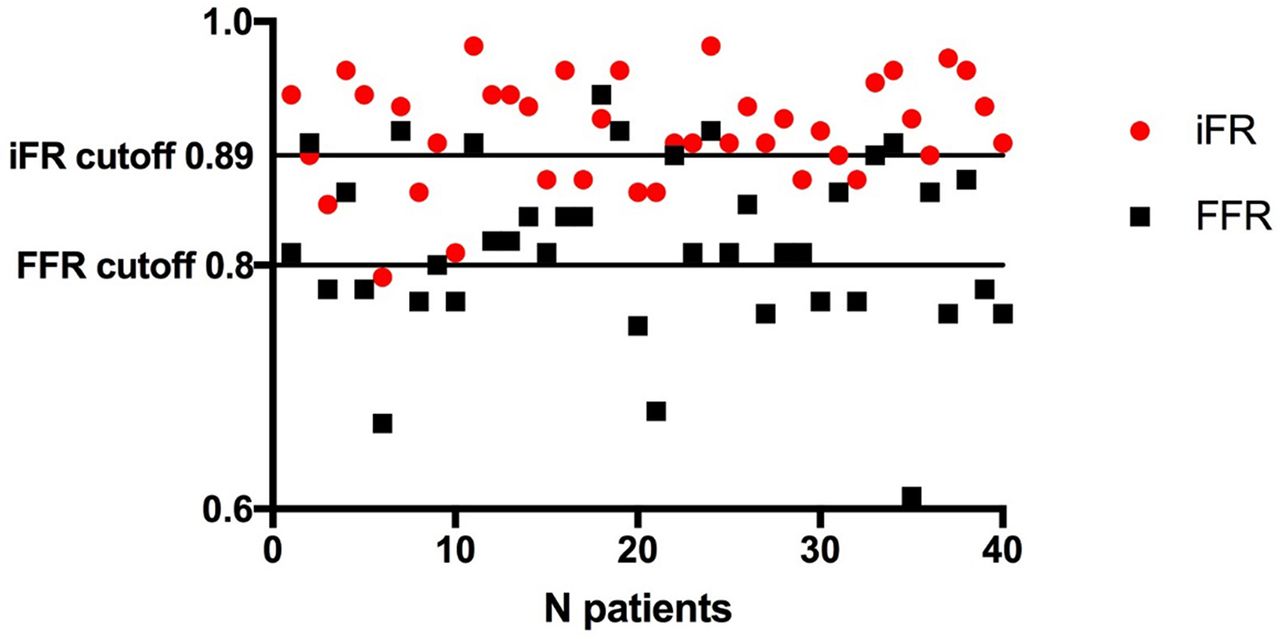
FFR vs iFR correlation
Results and conclusions A total of 40 patients were included in the study. Of the 40 patients there was discordance in the iFR and FFR measurements noted in 9 patients (22.5%). 7 patients were negative when initially studied with iFR (mean 0.92) and subsequently had positive FFR measurements mean (0.73). 2 patients were initially positive with iFR (mean 0.89) and subsequently had negative FFR studies (mean 0.87).
Implications The use of pressure wire measurements to assess intermediate lesions is a valuable tool available to cardiologists. The advancement in technology and the introduction of iFR allows quicker assessment of lesions as well as almost real-time assessment of multiple vessels and sequential lesions and improved patient comfort as well as reduced costs. This technology has been validated in large randomized control trials, however there exists an approximately 20% discordance in FFR and iFR measurements which can have implications for revascularization strategy. As iFR becomes more ubiquitous, clarity on how to best assess intermediate lesions is important. Our study highlights this discordance and demonstrates that whilst technological innovation is always welcome, a clear understanding of the technology and how to deal with any potential results is crucial.