Article Text

Statistics from Altmetric.com
Heart failure (HF) is the most common and serious cardiovascular complication of cancer therapy. As succinctly stated in an editorial by Lyon, ‘Success in the diagnosis and treatment of many cancers has resulted in a growing population of people living either cured of cancer or with their cancer controlled as a chronic disease by long-term treatment. This success story in modern medicine has created a new problem with some survivors developing cardiovascular disease (CVD) as a result of their cancer treatment.’1
CVD outcomes in patients with HF induced by cancer therapy are addressed in this issue of Heart.2 Comparing 75 patients with HF induced by cancer therapy (anthracycline chemotherapy or chest irradiation) to 894 patients with HF due to other causes, cancer therapy patients were younger, had fewer CVD comorbidities and a higher left ventricular (LV) ejection fraction but more severe LV diastolic dysfunction. Global longitudinal strain and cardiopulmonary exercise testing results were similar in both patient groups. On multivariable Cox regression analysis, HF due to cancer therapy, compared with other HF patients, was associated with a higher risk of death (HR 2.64; 95% CI 1.53 to 4.55; p=0.001) and the composite endpoint of LV assistant device implantation, heart transplantation or all-cause mortality (HR 1.79; 95% CI 1.10 to 2.91; p=0.019) (figure 1).

Kaplan-Meier curves for death and composite endpoint. The composite endpoint was defined as the composite outcome of left ventricular assistant device implantation, heart transplantation or all-cause mortality. CTHF, cancer therapy-induced heart failure; NCTHF, non-cancer therapy-induced heart failure.
Putting this study in context, Lyon1 points out the long interval (mean 10 years) between cancer therapy and clinical HF, the heterogeneous causes of HF in the comparison cohort, and the possibility that patients seen at a tertiary medical centre may have more advanced disease than in the general community. Even so, these data suggest that patients who present with HF late after cancer therapy have more severe HF and a poor prognosis. Looking ahead, he recommends that steps to prevent HF after cancer therapy should include (1) baseline CVD risk assessment, (2) close surveillance during therapy, (3) consideration of other options to reduce anthracycline cardiotoxicity, including lower doses or alternate agents and (4) routine long-term CVD surveillance after completion of cancer therapy.3 ‘Education of survivors to recognise cardiac symptoms and seek medical attention, and education of primary care physicians to consider cardiac late effects in cancer survivors are also important.’ Even with newer cancer therapies, cardiotoxicity remains a clinical problem.4
There has been great interest in the idea that patients would be more likely to consistently take medications for CVD prevention if combined in a single pill that combines or a ‘polypill’. In a meta-analysis of three randomised clinical trials comparing single pill containing a statin, aspirin and an antihypertensive medication to usual care, Selak et al5 found that the polypill approach increased the number of patients achieving guideline targets for blood pressure (62% vs 58%, risk ratio (RR) 1.08, 95% CI 1.02 to 1.15) and low-density lipoprotein (LDL) cholesterol (39% vs 34%, RR 1.13, 95% CI 1.02 to 1.25), as well as antiplatelet therapy in those with a prior CVD event. (figure 2) All three guideline targets were achieved in more patients with the polypill approach (24% vs 19%), although it is puzzling that this effect was strongest in those taking fewer pills at baseline.

Achievement of all threed treatment targets simultaneously at 12 months by subgroup. a,bRR and p value (heterogeneity) estimated from log-binomial regression model. cStatin, antiplatelet and >2 BP-lowering medications; all were indicated according to the participant’s physician on trial entry. dAntiplatelet target only applicable to people with established CVD. BP, blood pressure; CVD, cardiovascular disease; RR, risk ratio.
Ibañez et al6 point out that while patients with an acute CVD event now are likely to survive, there is a high risk of recurrent events, with about 9% of those events related to poor adherence to medical therapy. Recent studies show that major adverse CVD events are significantly lower in patients who actually take their medications so there clearly is a need to consider strategies to improve adherence. They conclude that ‘there is robust evidence that the use of a cardiovascular polypill strategy results in increased adherence to treatments, to better control modifiable risk factors and to a higher proportion of patients meeting European Society of Cardiology guideline targets for LDL cholesterol and blood pressure. Although there are still no data showing that these benefits translate into a reduction in hard endpoints, adoption of this strategy can now be considered in daily practice.’
Another paper in this issue of Heart used a large electronic primary care database in the UK to show that the age-standardised and sex-standardised prevalence of atrial fibrillation (AF) increased from about 2% in 2000 to over 3% in 2016.7 Over this time period the proportion of patients with AF treated with anticoagulants increased from 35% to 76% in those at high risk of stroke and from 33% to 47% in those at moderate risk of stroke. Conversely, use of anticoagulants appropriately decreased from 20% to 10% in patients with AF at low risk of stroke (figure 3). What accounts for this remarkable improvement in stroke prevention in patients with AF? Sandhu and Ezekowitz8 suggest several possible explanations, in addition to guideline changes, including the availably of newer oral anticoagulant medications, financial incentives for optimal AF management, integration of guidelines in clinical flow and use of standardised order forms. Going forward, they argue that ‘additional simple and cost-effective strategies are needed to demonstrate an even higher use of direct oral anticoagulant (DOAC) in eligible patients, particularly those at moderate risk, minimise overtreatment and reduce practice variations that can be implemented in different healthcare systems where incentivising may not be an option.’
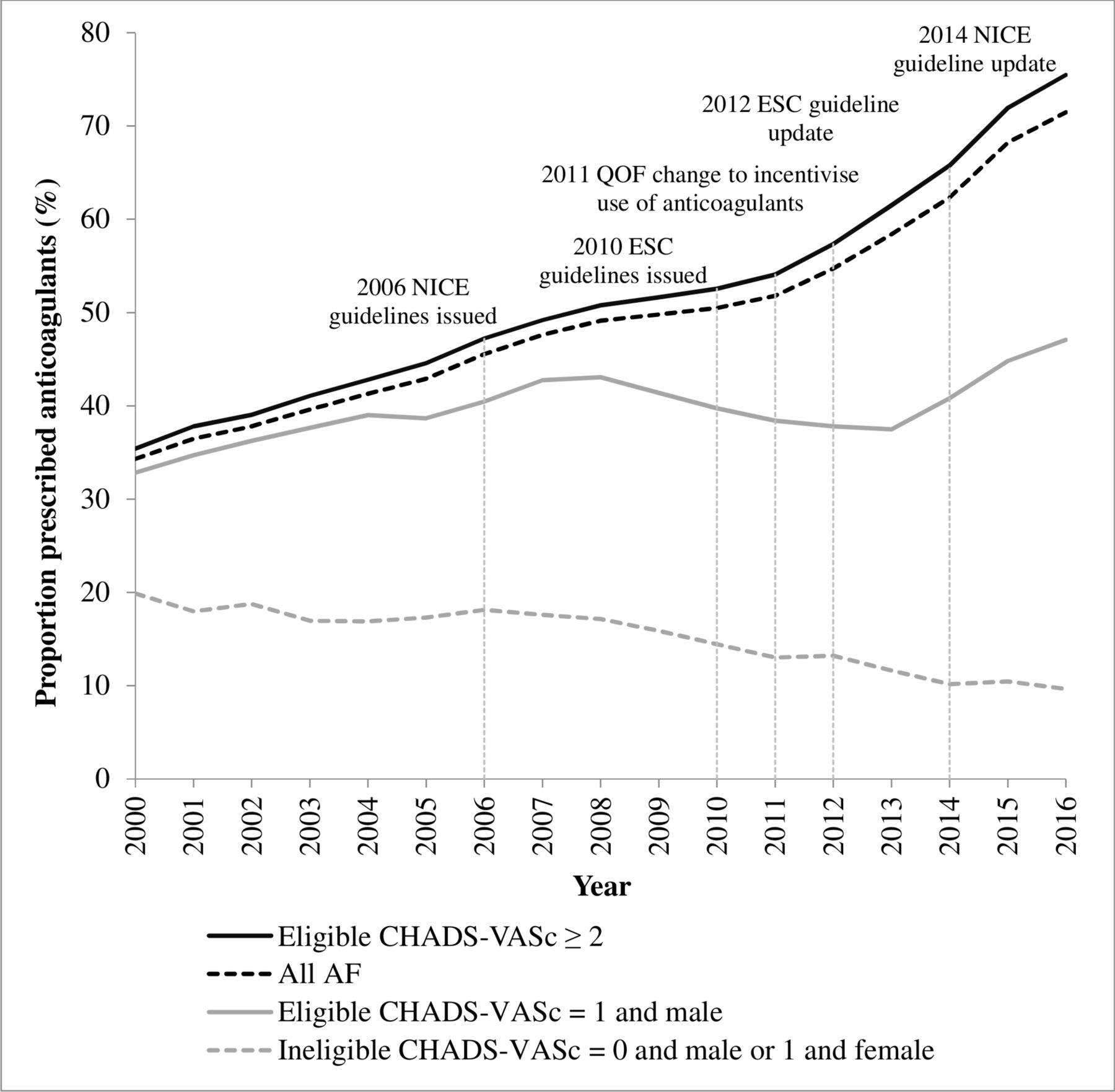
Proportion of patients with AF prescribed anticoagulants stratified by CHA2DS2-VASc score, 2000–2016. AF, atrial fibrillation; ESC, European Society of Cardiology; NICE, National Institute for Health and Care Excellence; QOF, Quality and Outcomes Framework.
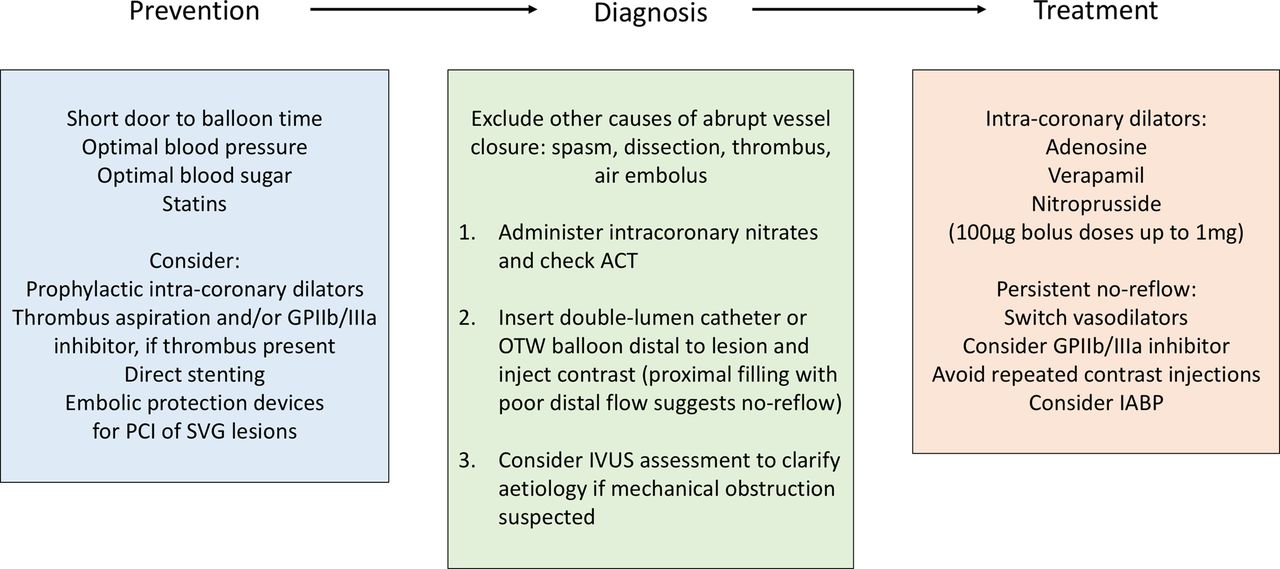
The Education in Heart article in this issue focuses on complications of percutaneous coronary interventions with descriptions of common complications and a summary of strategies to avoid and treat complications to improve the overall safety of percutaneous coronary intervention9 (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Management of no-reflow. ACT, activated clotting time; GPIIb/IIIa, glycoprotein IIb/IIIa; IABP, intra-aortic balloon pump; IVUS, intravascular ultrasound; OTW, over the wire; PCI, percutaneous coronary intervention; SVG, saphenous vein graft.
The image challenge case in this issue will test your interpretation of the ECG and echocardiogram in a 76-year-old man with progressive dyspnoea.10
Footnotes
Patient consent for publication Not required.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.