Article Text

Statistics from Altmetric.com
The primary goal of pre-participation cardiac evaluation in athletes is to identify individuals at high risk of sudden death but other cardiac abnormalities may be discovered. Athletes tend to have larger aortic dimensions than sedentary controls however it is unclear if this represents an aortopathy or is a normal physiological response to physical conditioning. To better understand the clinical implications of an enlarged aortic root in young athletes, Gati and colleagues1 compared aortic size and clinical outcomes in 3781 athletes with no evidence of a genetic aortopathy (mean age 19 years, 63% male) to 806 control subjects. This study found an enlarged aortic diameter in only 0.3% of athletes with no evidence of progressive enlargement over 5 years of follow-up. (figure 1)

Absolute aortic root dimensions in athletes and controls.
In an editorial, Jorstad and Groenink2 concur with the author’s conclusion that there appears to be little effect of physical activity on aortic size in young athletes without an underlying connective tissue disorder. The two other points they emphasise are that1 (1) reproducibility of aortic root measurements is not ideal and needs to be considered in patient follow-up and2 (2) pathological aortic dilation most often occurs in older individuals raising the concern that athletic activity as a teenager or young adult might affect aortic size decades later. They conclude that: ’While a liberal approach is probably warranted in the young athlete with mild aortic root dilatation, clinicians should remain vigilant in athletes at the end of their sports career and in later life. Prospective, longitudinal data are needed across a wide variety of sports and ages for further understanding the interaction between health and sports and to identify those individuals in whom too much of a good thing, in this case sports, might actually be a bad thing.'
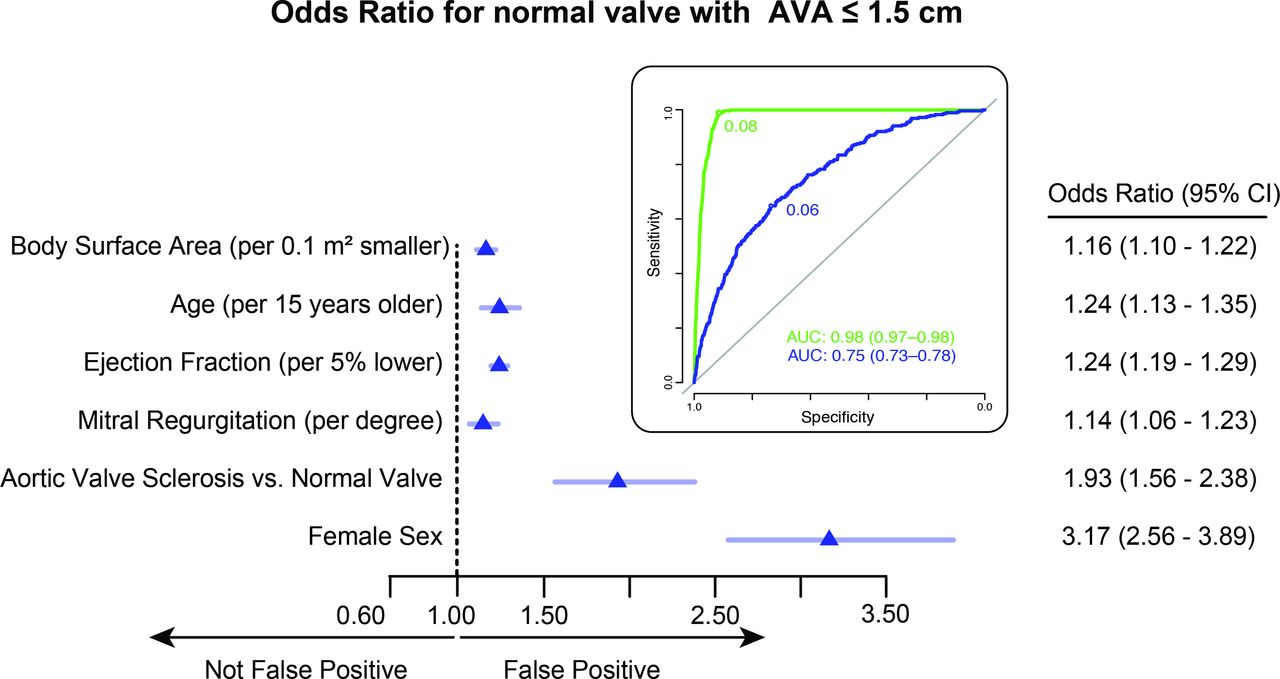
A diagnosis of low-gradient severe aortic stenosis (AS) has become more common in recent years based on the concept that velocity and gradient will not be elevated, even when aortic valve area (AVA) is small, if transaortic volume flow rate is low. A study in this issue of Heart by Mansilla and colleagues3 raises some concerns in diagnosing low-flow, low-gradient severe AS based on data from over 16 thousand echocardiograms. Aortic valve anatomy and flow were normal in 51%, aortic sclerosis (abnormal leaflets but velocity <2.5 m/s) was present in 40% and aortic stenosis in 1% of subjects. However, an AVA<1.5 cm2 was present in 0.5% of those a normal valve and 1.8% with a sclerotic valve despite the absence of valvular outflow obstruction (VOO). Factors associated with a small AVA but no VOO were a smaller body size, older age, lower ejection fraction, more mitral regurgitation, aortic sclerosis and female sex. (figure 2)

Predictors of small AVA values in studies without VOO. Multivariate logistic regression predictors of an AVA ≤1.5 cm2 in studies without VOO. ORs and 95% CI and cutoffs are shown for the model obtained in the learning dataset (n=9656) without entering SV and aortic TVI in the model. Insert: ROC curves, cutoffs and AUC obtained in the testing dataset (n=4974) for this model (blue) and for the one described in the online supplementary table 1, obtained forcing SV and aortic TVI into the model (green). AUC, area under the curve; AVA, aortic valve area; ROC, receiver operating characteristic; TVI, time–velocity integral; VOO, valvular outflow obstruction.
In the accompanying editorial Minners4 points out that these findings are congruent with the recent database study by Bradley and colleagues5 that also showed a low predictive valve of AVA for diagnosis of severe AS. The effects of small body size, low flow rates and measurement error all need to be taken into consideration. It also is noteworthy that numerous clinical outcome studies support the validity of a high aortic velocity, not a small AVA alone, for prediction of clinical outcome. Minners suggests that paying more attention to the ratio of the subaortic outflow velocity to aortic velocity, as originally proposed by Otto in 19866, might avoid apparent discrepancies between measures of AS severity in clinical practice.7 “In summary, the present paper emphasises that, in the framework of currently accepted cut-off values, relying on AVA in isolation tends to overestimate stenosis severity. The findings support an integrated approach in the assessment of AS severity as outlined in current guidelines.'
Another interesting paper in this issue is the systematic review and meta-analysis by Hernandez and colleagues8 looking at potential efficacy of low-sodium salt substitutes (LSSS) for reduction of adverse cardiovascular (CV) outcomes.8 Data from 21 randomised controlled clinical trials including over 7000 subjects showed that LSSS, compared with the control diet, reduced systolic blood pressure by about 8 mm Hg on average, increased urinary potassium and calcium excretion and decreased urinary sodium excretion. However, there was no demonstrable effect on the prevalence of hypertension, overall mortality, lipid or glucose levels, or body mass index. (figure 3) Unfortunately, the quality of evidence was very low for most outcomes suggesting that larger controlled clinical trials are needed to clarify whether this dietary approach is effective for reducing cardiovascular disease events.
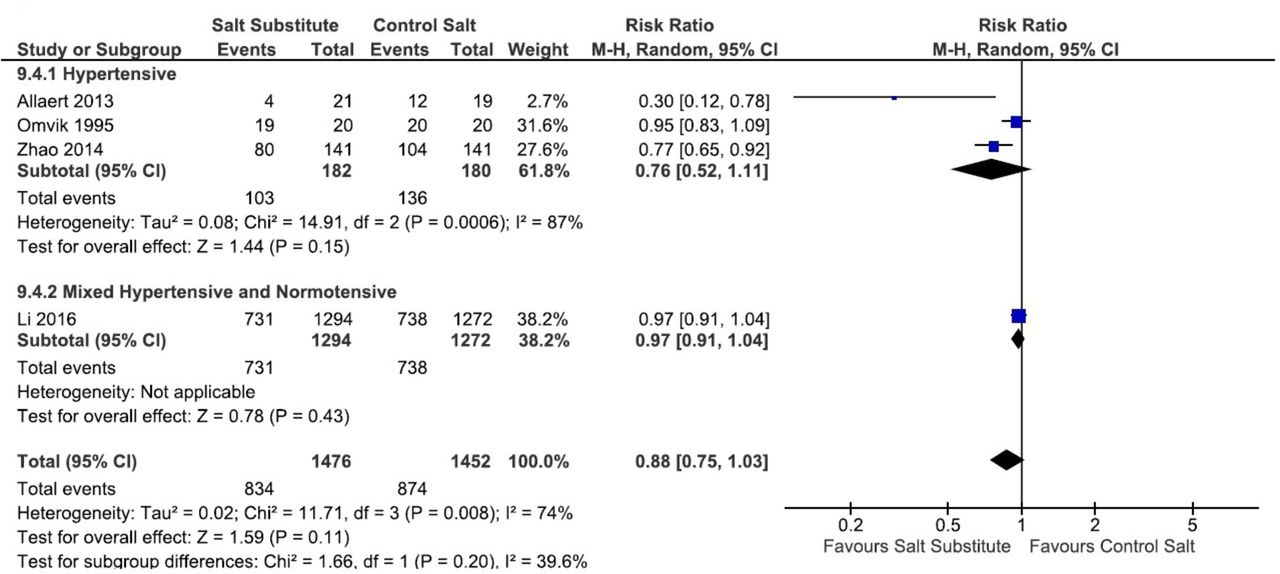
Effect of salt substitutes on detected hypertension. M-H, Mantel-Haenszel method.
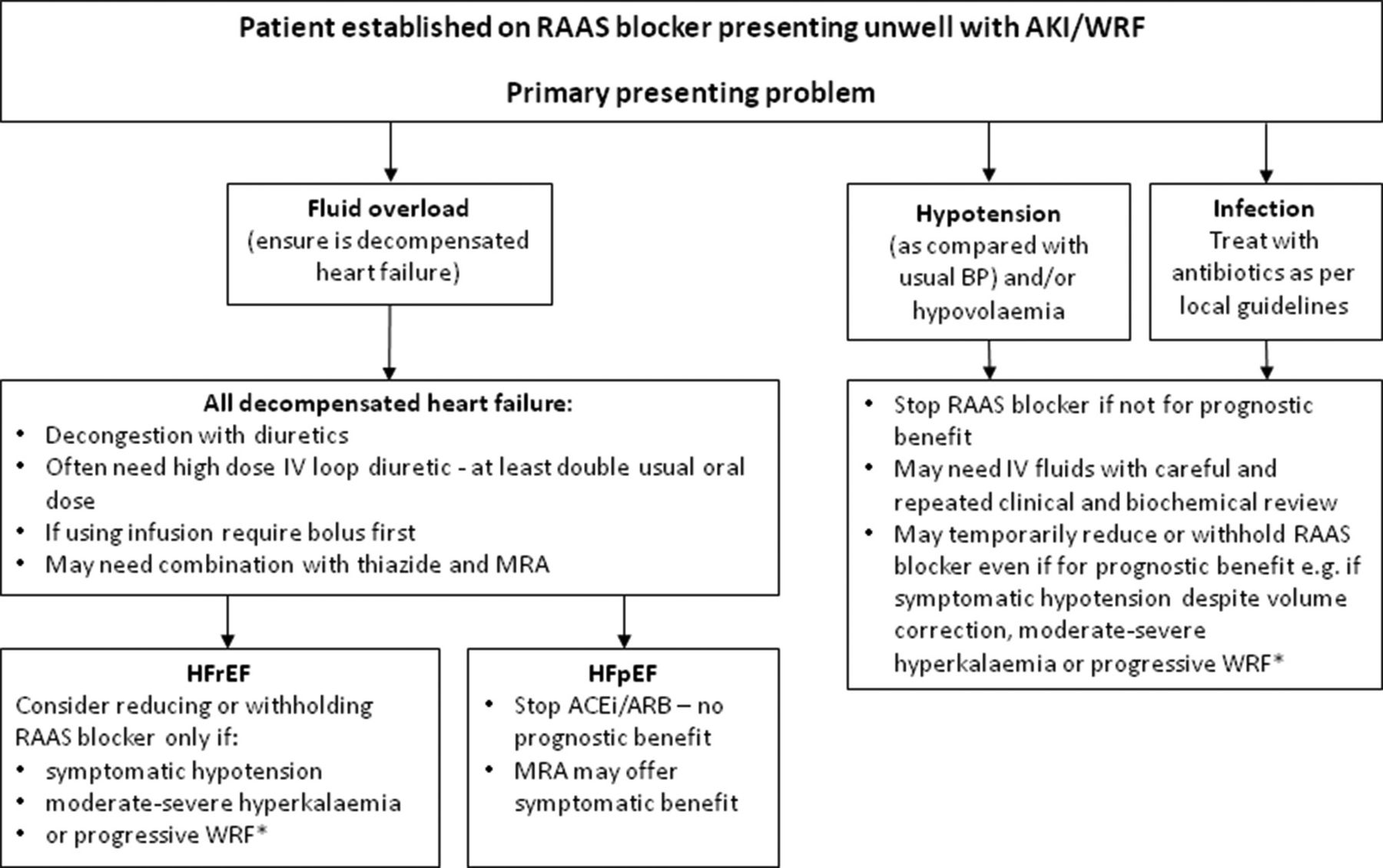
Management of renal dysfunction in adults with heart failure is a clinical challenge, especially given the potential adverse renal effects of inhibitors of the renin-angiotensin-aldosterone (RAAS) system. A concise national guidance statement from the British Society for Heart Failure and Renal Association in this issue of Heart provides useful guidance for clinicians. (figure 4)9
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Management of patients with acute kidney injury or worsening renal function who are receiving RAAS inhibitors. Clinical assessment of the individual patient is key. In all cases consider original indication for RAAS inhibitor. Major prognostic benefit: heart failure with reduced ejection fraction (HFrEF), post myocardial infarction (MI) and left ventricular systolic dysfunction, chronic kidney disease and albuminuria. No/little prognostic benefit: hypertension (other drug options available, heart failure with preserved ejection fraction (HFpEF). ACEi, ACE inhibitor ARB, angiotensin receptor blocker BP, blood pressure MRA, mineralocorticoid receptor antagonists WRF, worsening renal function.
The Education in Heart article in this issue10 summarises the current approach to management of infections of cardiac implantable electronic devices. Key messages are the increasing incidence of this highly morbid infection as more older adults are treated with permanent pacer devices, the importance removal of the entire system to eradicate infection, and the need for an experienced team to ensure a low rate or adverse events at the time of device removal.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.
Patient consent for publication Not required.