Article Text

Abstract
Objectives Electrocardiographic bundle branch block (BBB) is common but the prognostic implications in primary care are unclear. We sought to investigate the relationship between electrocardiographic BBB subtypes and the risk of cardiovascular (CV) outcomes in a primary care population free of major CV disease.
Methods Retrospective cohort study of primary care patients referred for electrocardiogram (ECG) recording between 2001 and 2011. Cox regression models were used to estimate hazard ratios (HR) as well as absolute risks of CV outcomes based on various BBB subtypes.
Results We included 202 268 individuals with a median follow-up period of 7.8 years (Inter-quartile range [IQR] 4.9–10.6). Left bundle branch block (LBBB) was associated with heart failure (HF) in both men (HR 3.96, 95% CI 3.30 to 4.76) and women (HR 2.51, 95% CI 2.15 to 2.94) and with CV death in men (HR 1.80, 95% CI 1.38 to 2.35). Right bundle branch block (RBBB) was associated with pacemaker implantation in both men (HR 3.26, 95% CI 2.74 to 3.89) and women (HR 3.69, 95% CI 2.91 to 4.67), HF in both sexes and weakly associated with CV death in men. Regarding LBBB, we found an increasing hazard of HF with increasing QRS-interval duration (HR 1.25, 95% CI 1.11 to 1.42 per 10 ms increase in men and HR 1.23, 95% CI 1.08 to 1.40 per 10 ms increase in women). Absolute 10-year risk predictions across age-specific and sex-specific subgroups revealed clinically relevant differences between having various BBB subtypes.
Conclusions Opportunistic findings of BBB subtypes in primary care patients without major CV disease should be considered warnings of future HF and pacemaker implantation.
- electrocardiography
- heart failure
- pacemakers
- cardiac risk factors and prevention
Statistics from Altmetric.com
Introduction
The use of surface 12-lead electrocardiogram (ECG) often results in identification of bundle branch block (BBB), even in individuals free of known cardiopulmonary disease. BBB comprises the subtypes incomplete right bundle branch block (IRBBB), right bundle branch block (RBBB), left bundle branch block (LBBB) and non-specific intraventricular conduction defect (NIVCD). BBB subtypes have been associated with an adverse prognosis in patients with known cardiovascular (CV) disease and in people recruited from the general population with and without CV disease.1–5
In the primary care setting, patients are referred for 12-lead standard ECG recording based on a broad range of indications, ranging from typical symptoms of CV disease to more diffuse symptoms as well as monitoring of medical treatment (eg, QTc interval-prolonging drugs) or as part of a routine health check. Opportunistic ECG recordings will often result in identification of various BBB subtypes. However, to the best of our knowledge, there are no clear and uniform recommendations or available risk prediction models aimed at handling and informing general practice patients who present with a potentially asymptomatic BBB subtype.
To address this, we used a middle-aged and elderly primary care population free from major CV disease, to (1) Estimate prevalences of BBB. (2) Describe associations between BBB subtypes and CV outcomes. (3) Test if the BBB subtypes are clinically useful in improving risk prediction of CV events. (4) If so, to develop a model useful in risk prediction of CV events in primary care patients with different BBB subtypes.
Methods
Study population
The present study is a part of the Copenhagen ECG study, comprising all individuals referred for ECG recording at the Copenhagen General Practitioners’ Laboratory (CGPL) between 2001 and 2011. CGPL is a centralised core facility used by general practitioners in the area of Copenhagen for the purpose of conducting various clinical examinations including ECG recording, as described previously.6–8
Individuals were excluded if they, at the time of inclusion (date of first ECG recording), were <40 years of age, had a pacemaker or implantable cardioverter-defibrillator, had an ECG unsuitable for measurement (see section on electrocardiography) or had a history of myocardial infarction (MI), atrial fibrillation (AF), ischaemic stroke, heart failure (HF) or valvular heart disease. We chose to exclude individuals <40 years of age due to a very low event rate and consequently low statistical power.
Baseline variables and outcomes
Using Danish administrative healthcare registers and a unique personal identification number assigned to all persons with permanent residence in Denmark, we followed individuals over time with respect to death, emigration, use of prescription drugs and any hospital, or outpatient clinic diagnoses. We identified baseline variables regarding comorbidity and medication status as described in detail previously.6–8 In brief, diabetes was defined as a register diagnosis of diabetes mellitus or treatment with glucose-lowering drugs. MI, AF, HF, pacemaker implantation, valvular heart disease and ischaemic stroke were defined from hospital discharge diagnoses and procedure codes in the Danish National Patient Registry. Hypertension was defined as a register diagnosis of hypertension or simultaneous treatment with two types of antihypertensive medication prior to or at inclusion. Finally, we constructed the Charlson Comorbidity Index which is a score combining several disease-specific comorbidities; for a list of included codes see online supplementary table 1.9 Our end points of interest were incident HF, MI, pacemaker implantation, AF, CV death and death from all causes. For a list of diagnostic codes see online supplementary table 2. The use of Danish administrative registers ensures complete nationwide coverage. Thus, we were able to interpret all cases of values not observed as not present and could define all variables without missing values.
Supplemental material
Electrocardiography
All ECGs were digitally recorded and stored in the MUSE Cardiology Information System (GE Healthcare, Wauwatosa, Wisconsin, USA) and were processed using version 21 of the Marquette 12SL algorithm.8 We excluded ECGs with rhythms different from sinus rhythm and other findings not suitable for the study analyses (eg, advanced atrioventricular block, delta waves, pace spikes, ventricular rates <30 beats per minute and >120 beats per minute). We defined BBB subtypes according to the American Heart Association (AHA), American College of Cardiology Foundation (ACCF), and Heart Rhythm Society (HRS) recommendations for standardisation and interpretation of the ECG implementing a few minor modifications as the 12SL algorithm cannot directly measure a notch or slur in the R-wave.10
Complete RBBB was defined as: (1) QRS duration >120 ms. (2) rsr’, rsR’ or rSR’ in leads V1 and/or V2. (3) S wave of greater duration than R wave or >40 ms in leads I and V6. (4) Normal R peak time in leads V5 and V6 but >50 ms in lead V1. Incomplete RBBB was defined by a QRS duration between 110 ms and 120 ms with other criteria being the same as for complete RBBB. LBBB was defined accordingly as: (1) QRS duration >120 ms. (2) Broad R wave in leads I, aVL, V5 and V6. (3) Absent Q waves in lead I, V5 and V6. (4) R peak time >60 ms in leads V5 and V6 but normal in leads V1, V2 and V3. NIVCD was defined as QRS duration >120 ms without meeting the criteria of RBBB or LBBB. Left ventricular hypertrophy was defined according to the Sokolow-Lyon ECG criteria.11
To verify that the algorithm used to identify BBB correctly captured the various BBB subtypes and not artefacts, premature ventricular contractions or paced rhythms despite the various applied filters, we randomly sampled 50 ECGs from each BBB category for manual evaluation. We found that all sampled ECGs (n=200) were correctly assigned by the algorithm in agreement with the defined BBB criteria.
Statistical analysis
Association analysis
Cox regression was used to assess the association of RBBB, IRBBB, LBBB and NIVCD with the hazard of incident HF, MI, pacemaker implantation, AF, CV death and all-cause mortality using individuals without the BBB subtype in question as reference. In case of a significant association between any of the BBB subtypes and an outcome of interest, we further tested the association between QRS duration, measured as a continuous variable, and the event within subjects with the specific BBB subtype.
Time-on-study was used as time scale in all survival analyses. All Cox models were adjusted for the following covariates obtained at baseline: age, hypertension, diabetes mellitus, a categorical variable of Charlson Comorbidity Index (0, 1, >2 points) and left ventricular hypertrophy. As many CV diseases are known to present differently across the two sexes, all analyses were conducted separately in men and women.12 Follow-up began on the day of first ECG recording and ended in case of emigration, event of interest, death or on 31 December 2013, whichever came first. Proportional hazard assumptions were tested and accepted by evaluating log-log plots. We considered a two-sided p value <0.05 as statistically significant.
Absolute risk prediction
Risk predictions were performed in a competing risk setting by combining a Cox model for all-cause mortality with a Cox model of the outcome in question.13 Absolute risks were reported in a risk chart stratified by 10-year age groups, sex and comorbidity (yes vs no) defined as either a Charlson Comorbidity Score >1, hypertension or diabetes mellitus. Differences in time-dependent area under the receiver operating characteristics curve (AUC) were calculated to investigate the added discriminative value of BBB subtypes in risk prediction of CV outcomes.14 15 Data were split into a training and test set with 101 splits using randomly chosen seeds. Ultimately, the seed with the median AUC in the models without BBB was chosen. Model performance and calibration were evaluated and accepted using Brier scores and calibration plots showing the observed frequency versus the predicted risk.16 17 We calculated 10-year absolute risks and reported these only in outcomes in which there was a statistically significant increase (p<0.05) in AUC when adding BBB status to a conventional risk model of CV outcomes. Furthermore, as an example, the relationship between QRS duration and the 10-year risk of HF was depicted for the 60–69 years age group with LBBB and comorbidity.
Sensitivity analysis
To investigate whether the associations between BBB subtypes and the risk of HF could be due to patients already having manifest but yet undiagnosed disease at the time of their referral for ECG recording, we performed a landmark analysis, in which we only included individuals on study with event-free survival at 1 year of follow-up.18
Results
Study population
A total of 202 268 persons were eligible for inclusion. Baseline characteristics of the study population are provided in table 1. The median follow-up time for the total study population was 7.8 years (IQR 4.9–10.6). During follow-up, we identified 11 082 cases of incident HF, 7211 cases of incident MI, 2246 pacemaker implantations, 13 648 cases of incident AF, 9184 CV deaths and 36 520 deaths from all causes. For number of events per BBB subtype please see online supplementary table 3.
Baseline characteristics
Prevalence
We found that the prevalence of RBBB, LBBB and NIVCD increased with age in both sexes. IRBBB and RBBB were much more prevalent in men than women, whereas LBBB was more prevalent in women (figure 1).

Prevalence of bundle branch block (BBB) subtypes by sex and age groups. IRBBB, incomplete right bundle branch block; LBBB, left bundle branch block; NIVCD, non-specific intraventricular conduction defect; RBBB, right bundle branch block.
Association between BBB subtypes and CV outcomes
We found IRBBB only to be associated with an increased hazard of pacemaker implantation in women (hazard ratio [HR] 2.89, 95% CI 1.71 to 4.90, p<0.001) (figure 2).

Forest plots depicting multivariable-adjusted hazard ratios (HR) by bundle branch block (BBB) and sex (A, men. B, women) for the following outcomes: incident heart failure, myocardial infarction, pacemaker implantation, atrial fibrillation and cardiovascular (CV) death using individuals without the BBB in question as reference. IRBBB, incomplete right bundle branch block; LBBB, left bundle branch block; RBBB, right bundle branch block; NIVCD, non-specific intraventricular conduction defect.
We found that RBBB was associated with an increased hazard of HF in both men (HR 1.28, 95% CI 1.13 to 1.44, p<0.001) and women (HR 1.42, 95% CI 1.22 to 1.66, p<0.001) and conferred a small increased hazard of CV death in men only (HR 1.22, 95% CI 1.07 to 1.39, p=0.005), all with reference to men and women, respectively, without RBBB. Additionally, RBBB was associated with an increased hazard of pacemaker implantation in both sexes (figure 2).
LBBB was associated with a markedly increased hazard of HF in both men (HR 3.96, 95% CI 3.30 to 4.76, p<0.001) and women (HR 2.51, 95% CI 2.15 to 2.94, p<0.001) and a modest association to CV death in men (HR 1.80, 95% CI 1.38 to 2.35, p<0.001). Furthermore, we found that LBBB was associated with a small but statistically significant increased hazard of MI and pacemaker implantation in both sexes (figure 2).
We found that NIVCD conferred increased hazards of HF in both men (HR 2.36, 95% CI 2.11 to 2.64, p<0.001) and women (HR 2.79, 95% CI 2.46 to 3.17, p<0.001) as well as CV death for both men (HR 1.62, 95% CI 1.41 to 1.86) and women (HR 1.42, 95% CI 1.22 to 1.66, p<0.001) with reference to men and women, respectively, without NIVCD. Additionally, we found NIVCD to be modestly associated with increased hazards of MI and strongly associated with pacemaker implantation for both sexes (figure 2).
We found no statistically significant associations between any BBB subtype and incident AF.
Associations regarding all-cause mortality were generally in line with CV death but with attenuated effects (online supplementary figure S1).
QRS duration in BBB
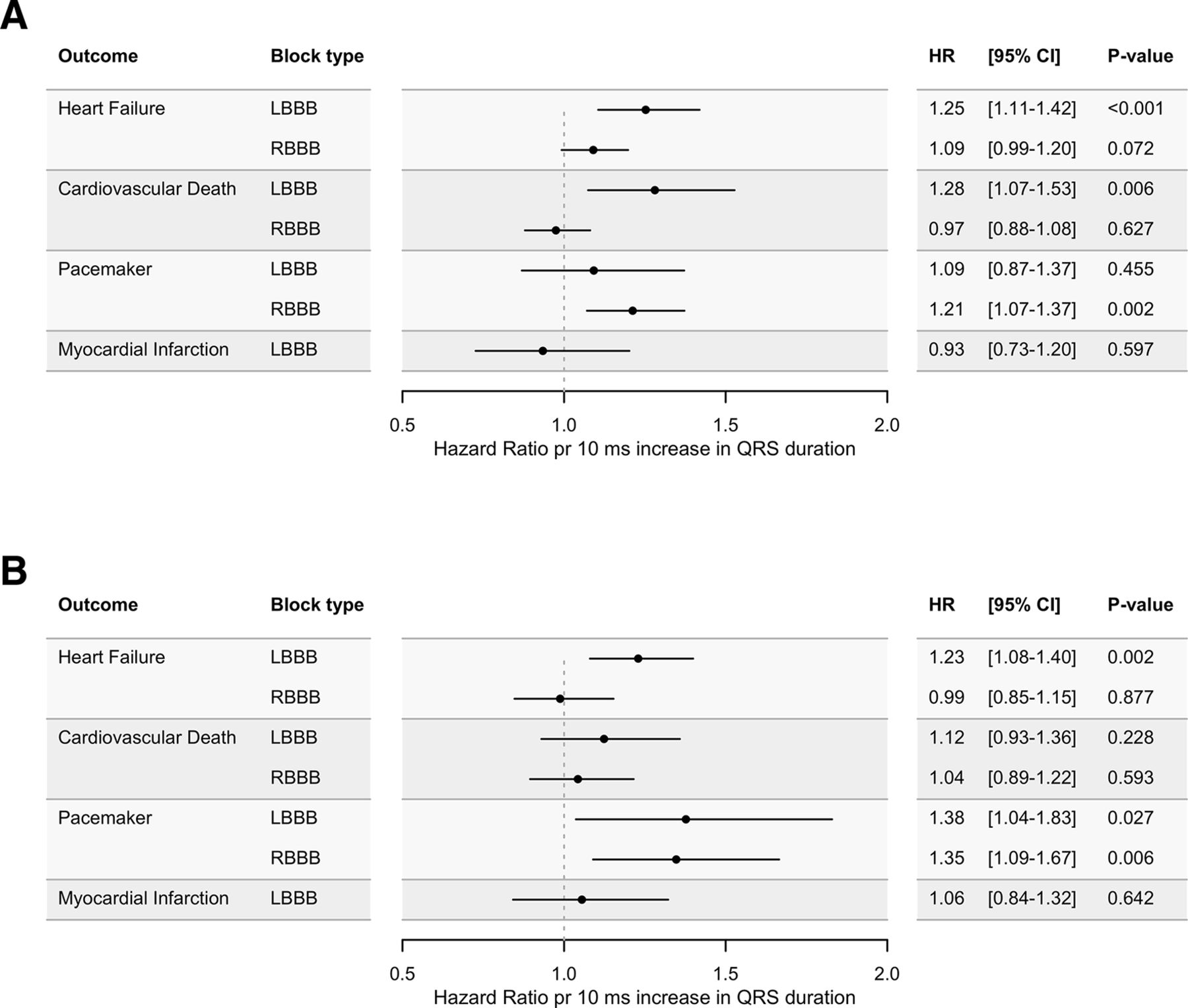
In individuals with LBBB, increasing QRS duration was associated with a statistically significant increased hazard of HF in both sexes and with an increased hazard of pacemaker implantation in women and CV death in men. In individuals with RBBB, we found that increasing QRS duration conferred an increased hazard of pacemaker implantation in both men and women (figure 3). Moreover, the 10-year absolute risk of HF increased almost linearly with QRS duration in the depicted age group (60–69 years) in both sexes with LBBB and comorbidity (figure 4).

Forest plots depicting hazard ratios per 10 ms increase in QRS duration in individuals(A, men. B, women) with bundle branch blocks. LBBB, left bundle branch block; RBBB, right bundle branch block.

Example of absolute 10-year risk of heart failure (HF) depicted by QRS duration in both men and women in the 60–69 years age category, with left bundle branch block (LBBB) and with comorbidity.
Risk prediction
We calculated AUC values for the conventional risk models as well as differences in AUC when adding BBB subtypes to the model for all outcomes stratified by sex. We found that the AUC was significantly increased for the 10-year prediction of HF in both men (0.83%, 95% CI 0.51 to 1.16, p<0.001) and women (0.64%, 95% CI 0.40 to 0.87, p<0.001) as well as for pacemaker implantation in both men (2.48%, 95 % CI 1.45 to 3.51, p<0.001) and women (2.44%, 95 % CI 1.40 to 3.48, p<0.001). For AUC values for the conventional models, changes in AUC for all outcomes, Brier scores, and calibrations plots please see online supplementary figure S2, online supplementary table 4 and online supplementary figure S3. For the full Cox models used for risk prediction, please see online supplementary table 5. Estimated absolute 10-year risks for pacemaker implantation and HF stratified by age group, sex and comorbidity are provided in figure 5.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Risk chart depicting 10-year absolute risks of HF and pacemaker implantation by age group, sex and block type. Risk estimates are stratified by the presence of comorbidity at time of ECG recording. BBB, bundle branch block; IRBBB, incomplete right bundle branch block; RBBB, right bundle branch block; LBBB, left bundle branch block; NIVCD, non-specific intraventricular conduction defect.
Sensitivity analysis
We performed 1-year landmark analyses for the outcome HF and found that the associations were only slightly attenuated compared with the main analyses (online supplementary table 6).
Discussion
In a large contemporary population of primary care patients free of major CV disease, we found (1) associations between several BBB subtypes and CV death, HF, MI and pacemaker implantation. (2) That increasing QRS duration was associated with an increased risk of incident HF in both men and women with LBBB and pacemaker implantation in men with LBBB as well as in men and women with RBBB. (3) That adding BBB subtypes to a conventional CV risk model improved 10-year risk prediction of HF and pacemaker implantation. (4) And finally, several BBB subtypes conferred clinically relevant differences in absolute risks of HF and pacemaker implantation.
We found relatively strong associations between LBBB, NIVCD and incident HF as well as strong associations between RBBB, LBBB, NIVCD and pacemaker implantation in both men and women. We also found modest associations between LBBB, NIVCD and MI in both men and women, between RBBB and HF in both men and women and between RBBB, LBBB, NIVCD and CV death in men as well as NIVCD and CV death in women. These findings are consistent with previous studies of BBB in the general population.3 4 19–22
While an association between a biomarker of interest and an outcome on a population level can help inform biology or generate hypothesis about causality, an association does not necessarily translate into clinically meaningful risk prediction for the individual patient.23 Accordingly, we first tested whether adding BBB subtypes to a conventional CV risk model improved risk prediction of selected CV events and found a significant improvement in AUC for HF and pacemaker implantation. In our setting, AUC corresponds to the probability that a person who experiences an event of interest within 10 years of follow-up receives a higher predicted risk than a person who is alive and does not experience the event.24 For the outcomes pacemaker implantation and HF where we found improvements in AUC, we went further and estimated absolute risks of having various BBB subtypes (figure 5).
We found that both LBBB and NIVCD conferred very high 10-year risks of HF in both sexes. For example, we predicted a 65-year-old male with one or more comorbidity (eg, hypertension) and LBBB to have a 32% 10-year risk of HF compared with only 10% if he had no BBB. Based on our findings, we suggest that primary care patients with LBBB or NIVCD, not already treated for or diagnosed with HF, should be referred for further CV evaluation and echocardiography because these BBB subtypes are likely to represent either an yet unrecognised failing heart or an individual at a very high risk of a future HF event.
In men and women with RBBB, we found each unit increase in QRS duration associated with an increasing hazard of pacemaker implantation. These findings suggest that the broader the RBBB QRS-complex is, the more likely it is that other parts of the conduction system are affected. For LBBB, we observed that increasing QRS duration was associated with increased risks of incident HF in both sexes. In patients with mild HF, both LBBB as well as prolonged QRS duration have been associated with a poorer prognosis and decline in left ventricular ejection fraction (LVEF).25 26 Furthermore, in patients with LBBB, an inverse relationship between QRS duration and LVEF has been demonstrated.27 Thus, both the electromechanical dyssynchrony in the LBBB pattern as well as the magnitude of QRS duration seem to contribute to the ‘cardiac stress’ resulting in deterioration of the LVEF.
The newest recommendations do not advise routine ECG screening as a tool for risk stratification in asymptomatic individuals.28 However, even though we do not have access to the clinical indications for ECG recording, our data indicate that the ECG could be of value in identifying primary care patients with high risk of HF and pacemaker implantation. We provide a risk chart (figure 5) that can serve as an instrument for risk prediction.
Limitations
Different electrocardiographic definitions of BBB subtypes exist making study comparisons difficult; we chose to rely as closely as possible on the most recently available AHA guideline, which is somewhat restrictive.10 As such, certain types of NIVCD in our study would likely be interpreted as LBBB or RBBB in a clinical setting. The validity of many diagnoses in the registers is unknown but our definitions of HF, MI, AF, hypertension, and the diagnoses used in the Charlson Comorbidity Index have previously been validated with high positive predictive values.9 29 30 We did not have data on indication of why the ECG recording was performed but landmark analysis along with graphical evaluations of the proportional hazard assumptions indicated that the associations we observed were not driven by accumulation of events instantly after the ECG recording. This would have been expected if most patients were referred for ECG recording as a result of significant symptoms. The occurrence of AF in our study might be an underestimation due to the often paroxysmal nature of the arrhythmia. Patients could potentially have a sinus rhythm ECG recorded at study inclusion and already be suffering from yet undiagnosed AF or patients with incident AF never treated at a hospital could be overlooked.
Conclusion
Using a large primary care population, consisting of more than 200 000 individuals without major CV disease, we found that RBBB and NIVCD were much more prevalent in men than women and that LBBB was marginally more prevalent in women than men. We found significant associations between RBBB, LBBB, NIVCD and the hazard of incident HF, MI as well as pacemaker implantation. Absolute risk predictions of HF and pacemaker implantation revealed clinically relevant differences between having various BBB subtypes versus no BBB.
Key messages
What is already known on this subject?
Incidental discoveries of electrocardiographic bundle branch block (BBB) are frequent in primary care patients but the prognostic implications in a primary care population free of major cardiovascular (CV) disease remain unclear.
What might this study add?
We provide age-specific and sex-specific absolute risks of pacemaker implantation and heart failure (HF) for various BBB subtypes. Both left bundle branch block (LBBB) and non-specific intraventricular conduction defect (NIVCD) are associated with very high 10-year risks of HF in both sexes. Furthermore, in people with BBB, increasing QRS duration confers increased risk of HF.
How might this impact on clinical practice?
CV healthy middle-aged and elderly primary care patients with an incidental discovery of LBBB or NIVCD are at very high risk of HF and might benefit from referral for further CV evaluation and echocardiography.
References
Footnotes
PVR and MWS contributed equally.
Contributors Study concept and design were determined by: PVR, JBN, MWS, AGH. Acquisition of data was performed by: CG, AHP, JBN. Digital ECG analysis was performed by: PVR,JBN, CG, JM. Drafting of the manuscript was carried out by: PVR, MWS, JBN. Critical revision of the manuscript for important intellectual content was carried out by: JBN, MWS, JG, CG, AHP, MSO, SH, JHS, LK, JM, SH, CT-P, LK, AGH. Statistical analysis and data interpretation were performed by: PVR, MWS, JBN, JG. Fund raising was performed by: JBN, CG, SH, AGH.
Funding This study was supported by The Research Committee of Rigshospitalet and The John and Birthe Meyer Foundation. JBN was supported by the Danish Heart Foundation (16-R107-A6779), the Lundbeck Foundation (R220-2016-1434), the AP Møller Foundation for the Advancement of Medical Science and Fondsbørsvekselerer Henry Hansen og Hustru Karla Hansen Født Vestergaards Legat.
Competing interests AGH is an employee of Novo Nordisk A/S.
Ethics approval Due to no active participation from study subjects, no approval from an ethics committee was required according to Danish law. The use of register data was approved by the Danish Data Protection Agency.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no unpublished data from the study.
Patient consent for publication Not required.