Article Text

Statistics from Altmetric.com
In patients with an acute coronary syndrome (ACS), prehospital transmission of the ECG offers the potential to reduce the time delay between symptom onset and initiation of treatment. However, the effect of this telemedicine intervention on clinical outcomes has not been well validated. In a systematic review and meta-analysis, Marcolino and colleagues1 identified 30 non-randomised controlled and 7 quasi-experimental studies of telemedicine for ACS that included a total of almost 17 000 patients. In these studies, prehospital ECG transmission (compared with usual care) was associated with a lower in-hospital mortality (relative risk (RR) 0.63 (95% CI 0.55 to 0.72)), door-to-balloon time (mean difference −28 min (95% CI −35 to –20)), 30-day and long-term mortality (RR 0.61 (95% CI 0.40 to 0.92)) (figure 1). However, there was moderate to large heterogeneity for all these findings suggesting that more rigorous evaluation of telemedicine strategies for improving outcome is needed.

(A) Forest plot showing the risk of 30-day mortality in patients submitted to telemedicine strategies associated to usual care versus usual care. (B) Forest plot showing the risk of long-term mortality in patients submitted to telemedicine strategies associated to usual care versus usual care. LL, lower limit; RR, relative risk; UL, upper limit.
In an editorial, Bosson2 points out that this meta-analysis focused on prehospital ECG transmission with or without teleconsultation. She goes on the discuss the untapped potential of telemedicine for ACS and other cardiovascular conditions. ‘Telemedicine can allow for remote follow-up and close monitoring of patients, ensuring medication compliance and detecting early signs of decompensation before it results in additional complications and hospital readmission. Transmission of data from the patient’s home and the ability of the physician to evaluate the patient remotely can expand the possibilities for home-based care and improve patient quality of life. This is especially valuable in rural communities, where physician specialists are lacking and patients have long travel times to seek care. There are incredible opportunities for the use of telemedicine to improve patient outcomes that have yet to be realised.’
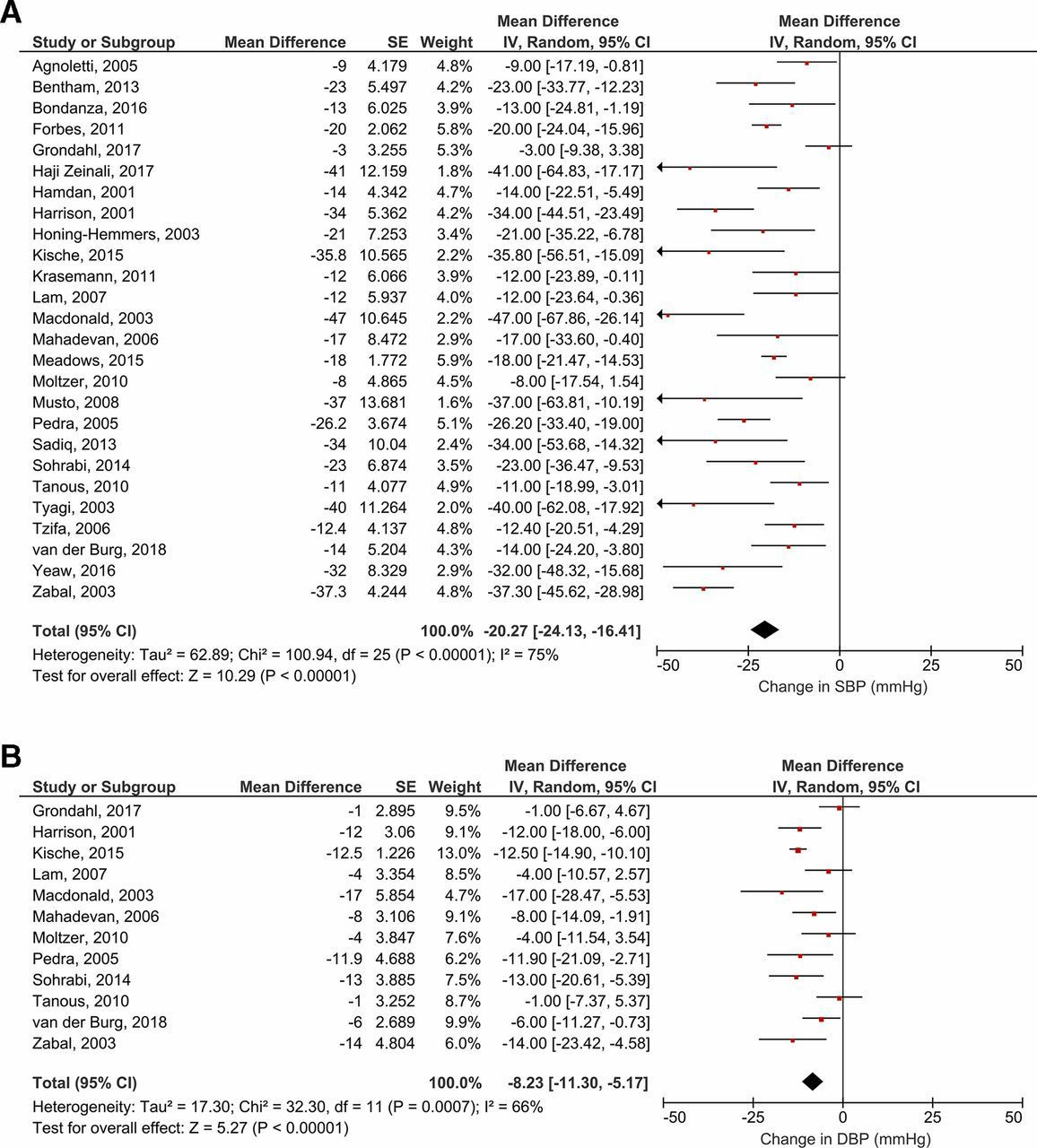
Long-term outcomes in patients with aortic coarctation are adversely affected by a high prevalence of hypertension. In a meta-analysis of 26 studies with 1157 patients undergoing stent implantation for aortic coarctation Meijs and colleagues3 found that systolic blood pressure (BP) was reduced by 20.3 mm Hg (95% CI 16.4 to 24.1) and diastolic BP by 8.2 mm Hg (95% CI 5.2 to 11.3) at medium term (about 2 year) follow-up (figure 2). There was a greater reduction in systolic BP at follow-up in those with stenting of a native coarctation and with a higher systolic BP and peak systolic gradient across the coarctation at baseline.

Forest plots showing the pooled mean change in SBP (A) and DBP (B) from baseline to last follow-up using a random-effects model. Data are presented as mean difference (mm Hg) and 95% CI. DBP, diastolic blood pressure; IV, inverse variance; SBP, systolic blood pressure.
In the accompany editorial, Butera4 points out that up to 30%–40% of patients with an aortic coarctation develop systemic hypertension long term, even with a successful relief of aortic obstruction by surgical or transcatheter intervention. This suggests there are other causes of hypertension in these patients. ‘Many abnormalities may be involved and they include impaired vascular function, hyper-activation of the renin–angiotensin system, autonomous nervous system imbalance, abnormal arterial compliance and abnormal activation of baroreceptors located in the convexity of aortic arch and in the carotid arteries.’ He proposes that ‘in some way, aortic coarctation could be considered as a systemic vascular disease of the pre-coarctation arteries’.
The potential value or renal denervation (RDN) for control of hypertension remains controversial, especially given the strong evidence that antihypertensive medical treatment reduces cardiovascular mortality and morbidity. However, long-term compliance with medical therapy is suboptimal so there may be a role for a non-pharmacological approach. In this issue of Heart, the Joint UK Societies’ 2019 Consensus Statement on Renal Denervation reviews the evidence for this approach and provides a research agenda for future clinical studies (figure 3).5 However, they recommend that RDN currently only be offered to patients in the context of a clinical trial.
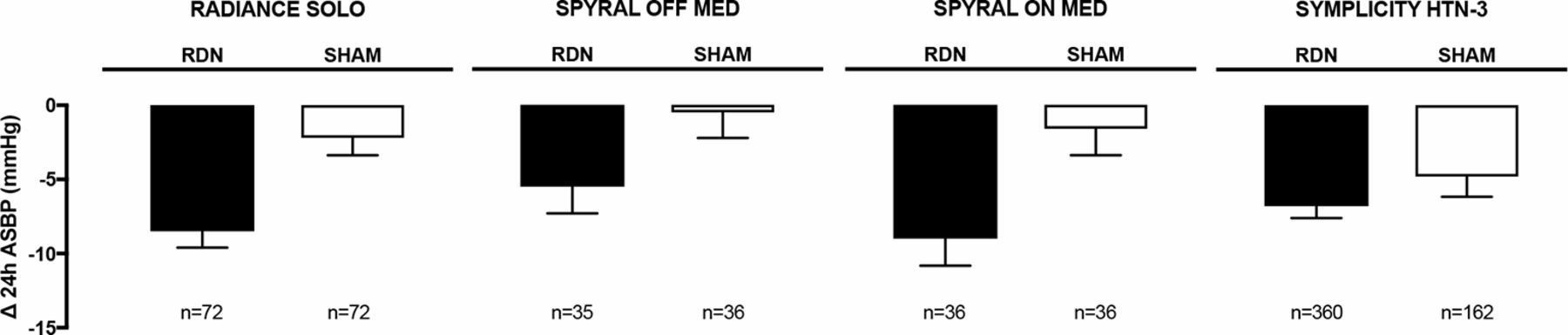
24 hours ASBP reduction in Spyral HTN-OFF Med and HTN-ON Med, RADIANCE-HTN solo and SYMPLICITY HTN-3 randomised clinical trials. Data are shown as mean±SEM. Δ, change from baseline; ASBP, ambulatory systolic blood pressure; RDN, renal denervation.
McGregor and Webb provide some perspective on the controversy surrounding RDN.6 They summarise previous clinical trials, including results and limitations, and conclude that although RDN leads to a sustained drop in BP, the magnitude of the effect appears to be modest (a decrease in systolic BP by about 6 mm Hg at 6 months). They conclude ‘significant questions remain about how effective RDN is in the long term, whether it may have harms that outweigh its benefits and how to identify those who will respond well to RDN. Until these questions can be answered, RDN will remain on trial’.
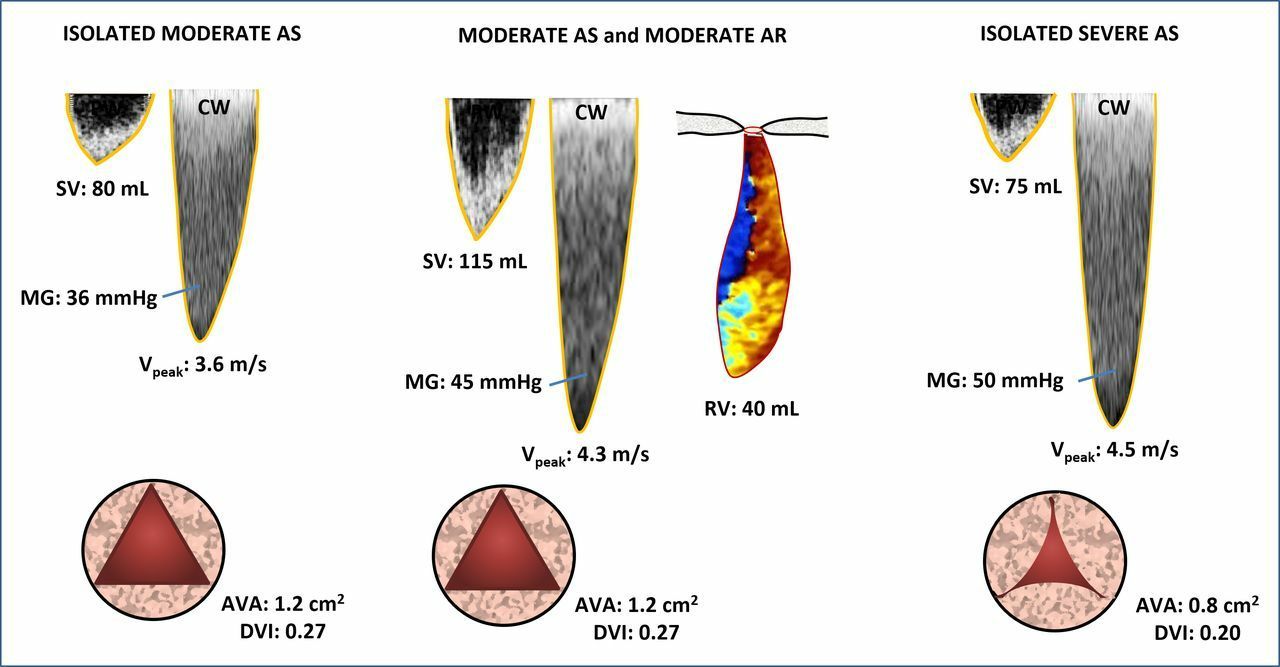
The Education in Heart article in this issue addresses the clinical issues surrounding patients with mixed aortic stenosis and regurgitation. Evaluation of these patients is based on consideration of multiple measures of disease severity and often requires integration of data from several imaging modalities (figure 4).7 Timing of intervention typically is guided by the effects of the predominant haemodynamic lesion. With balanced stenosis and regurgitation, clinical judgement is paramount given the paucity of evidence and lack of specific guidelines.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Haemodynamic interaction between AS and AR. This figure illustrates three scenarios: isolated moderate AS, isolated severe AS and concomitant moderate AS and moderate AR. In latter scenario, the regurgitant volume resulting from the moderate AR causes an increase in the LV stoke volume. In turn, this AR-related increase in forward stroke volume yields to an increase in the peak jet velocity and mean gradient for a given AVA. In this scenario, the peak aortic jet velocity and mean gradient overestimate the severity of the AS component but provide an adequate estimation of the overall haemodynamic severity of the combination of AS+AR. However, the AVA provides an adequate estimation of the severity of as but underestimates the overall severity of AS+AR. AR, aortic regurgitation; AS, aortic stenosis; AVA, aortic valve area; CW, continuous-wave Doppler; DVI, Doppler velocity index; MG, mean transvalvular pressure gradient; PW, pulsed-wave Doppler; RV, aortic regurgitant volume; SV, stroke volume; VPeak, peak aortic jet velocity. Figure artwork by MIA Pibarot.
Be sure to check out the Cardiology in Focus article in this issue on smart device apps every cardiologist should know.8 I think you will find many of them indispensable once you try them.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.