Article Text

Statistics from Altmetric.com
Many patients with severe symptomatic aortic stenosis (AS) present for medical care late in the disease course, at a time point when outcomes after surgical or transcatheter aortic valve replacement may not be optimal. The diagnosis of AS is often missed on physical examination by primary care providers.1 Even when an echocardiogram is obtained, discrepancies in measures of AS severity can lead to confusion and failure to refer patients for appropriate intervention. In an effort to use a systems-based approach to improving diagnosis of severe AS, Bradley and colleagues looked at the accuracy of echocardiographic measures of AS severity in over 77 thousand patients over a 4 year period in a single US-based healthcare organisation.2 A combined assessment, using peak velocity, mean gradient, and the dimensionless index (simpler surrogate for aortic valve area [AVA}), provided the best sensitivity (92%) and specificity (99%) for diagnosis of severe AS compared with any single measure alone. (figure 1)

Schematic of echocardiographic measures of aortic stenosis as the measurement of left ventricular outflow tract (LVOT) diameter is squared in the calculation of AVA, inaccuracies in this measurement can contribute substantially to error. The dimensionless index does not depend on the measurement of LVOT diameter. The present study suggests routinely captured data on aortic velocities, mean gradient, and dimensionless index are more accurate than AVA in the assessment of severe aortic stenosis when compared with the clinically relevant interpretation of the echocardiographic reader. AVA, aortic valve area; CW, continuous wave; DI, dimensionless index; VTI, velocity time integral.
In a provocative editorial, Baumgartner asks ‘Should we forget about valve area when assessing aortic stenosis?’.3 The major source of error in calculation of AVA is measurement of left ventricular outflow tract (LVOT) diameter and area. The dimensionless index ignores LVOT size and instead considers the simple ratio of LVOT to aortic velocity. In effect, this ratio is indexed for body size because LVOT size indicates the expected AVA for that patient, even during growth from birth to adulthood. Baumgartner concludes that “inclusion criteria identifying severe AS in research projects—particularly in retrospective analyses—must indeed be carefully revisited. Identification of severe AS by an echocardiographically reported valve area of <1.0 cm2 alone should not be acceptable.’ In my view, widespread acceptance of the dimensionless ratio (which was originally proposed in the same research papers as the Doppler continuity equation) would require a better name, as well as further outcome-based validation – my suggested new name is ‘aortic valve index’.
Resistant hypertension is a vexing clinical problem. In a meta-analysis of published data including over 3.2 million patients about 10% of patients had pseudo-resistant, so called ‘white coat’ hypertension, with normal blood pressure (BP) documented on home or ambulatory BP measurements. (figure 2)4 An additional 15% of patients were classified as apparent-treatment-resistant, who had not been fully evaluated for pseudo-resistant hypertension or medical non-compliance. However, there still was a 10% overall prevalence of true-resistant hypertension with an even higher prevalence in those with chronic kidney disease (23%), renal transplantation (56%) and the elderly (12%).

Meta-analysis results for prevalence of true resistant hypertension and pseudo-resistant hypertension.
In a thoughtful editorial, Mazarzadeh, Pinho-Gomes and Rahimi5 conclude that: “Noubiap et al 4 remind us that resistant hypertension affects a sizeable proportion of patients with treated hypertension, and about half of them have true resistant hypertension that requires more aggressive BP management to avoid the deleterious consequences of persistently elevated BP. The study also reveals that the concept of resistant hypertension, particularly ‘controlled’ resistant hypertension and the number of drugs used, may deserve to be revised in keeping with the recent decrease in diagnostic thresholds and multidrug low-dose treatment recommendations for hypertension’ (figure 3).
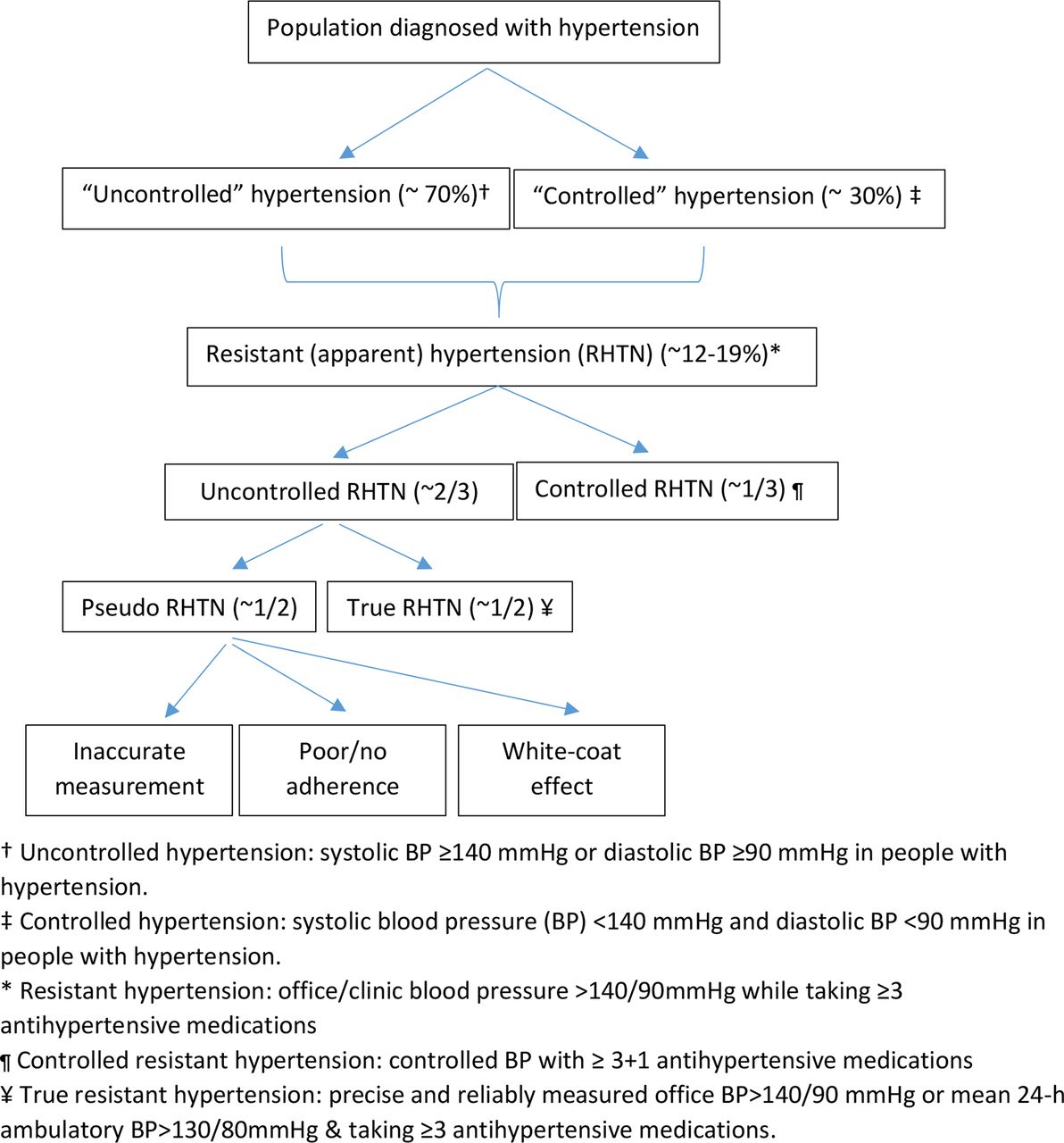
Flow chart of the definition of resistant hypertension. Percentages were approximately estimated from epidemiological studies conducted in the UK and the USA.
The benefits of cardiac rehabilitation (CR) for adults with coronary heart disease are undoubted but lack of access and cost of standard centre-based programmes limit this therapy to a minority of eligible patients. In a randomised study of standard CR versus remotely-monitored CR, the telemedicine approach was non-inferior to the standard CR approach as assessed by exercise status, maximum oxygen consumption, and waist and hip circumference at completion of the programme (figure 4).6 Programme and medication costs were lower for the telemedicine CR with no difference in hospitalisation costs. Lavie, Kachur and Milani7 congratulate the authors on this study and comment that “Certainly, more comprehensive Remote-CR models, including home, internet and community-based programmes, are needed to provide alternatives to conventional, medically supervised, facility-based Standard-CR. The time has come to ‘re-brand and re-invigorate’ “

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Remotely monitored exercise-based cardiac telerehabilitation platform schematic.
The Education in Heart article in this issue provides an overview of sexual function and cardiovascular disease, focused primarily on men, that will be useful to clinicians in their daily practice.8
Also in this issue, the Cardiology in Focus section includes an article about using twitter effectively to follow the cardiology literature and communicate with colleagues, especially during medical conferences.9 We welcome our new Cardiology in Focus section editors -- Clare Coyle, Sarah Hudson, and Victoria Stoll -- and look forward to many more interesting articles over the coming year.
Footnotes
Patient consent for publication Not required.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.