Article Text

Statistics from Altmetric.com
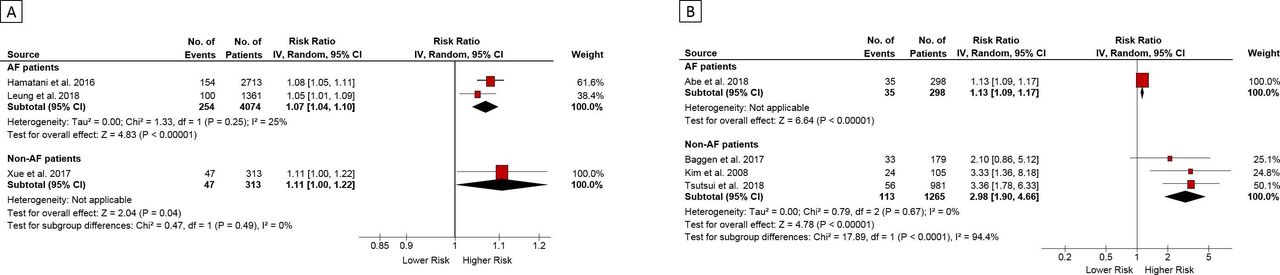
The association of left atrial (LA) enlargement, atrial fibrillation (AF) and adverse cardiovascular outcomes is well known. However, it remains unclear whether this association is simply related to AF or whether LA size also is an important prognostic variable. In a meta-analysis of over 50 000 patients from studies that included patients with (n=23) or without (n=68) AF, Froehlich and colleagues1 found stronger associations between LA size and cardiovascular outcomes in patients without compared with those with AF (figure 1). For example, a larger LA diameter was significantly associated with stroke and thromboembolic events (risk ratio (RR) 1.38, 95% CI 1.02 to 1.87; p=0.03) in patients without AF, but not in those with AF (RR 1.02, 95% CI 0.98 to 1.07; p=0.27; p for difference=0.05). The authors propose that these associations likely are due to LA size reflecting atrial myopathy even when AF is not present.

Association of LA diameter index and risk of cardiovascular outcomes. Association of LA diameter index with incident stroke or thromboembolic events (A) and major adverse cardiac events (B). Data are risk ratios with corresponding 95% CIs from inverse variance (IV)-weighted random-effects models. Meta-analysis results are separately presented as diamonds for studies including patients with AF and studies without patients with AF. AF, atrial fibrillation; LA, left atrial.
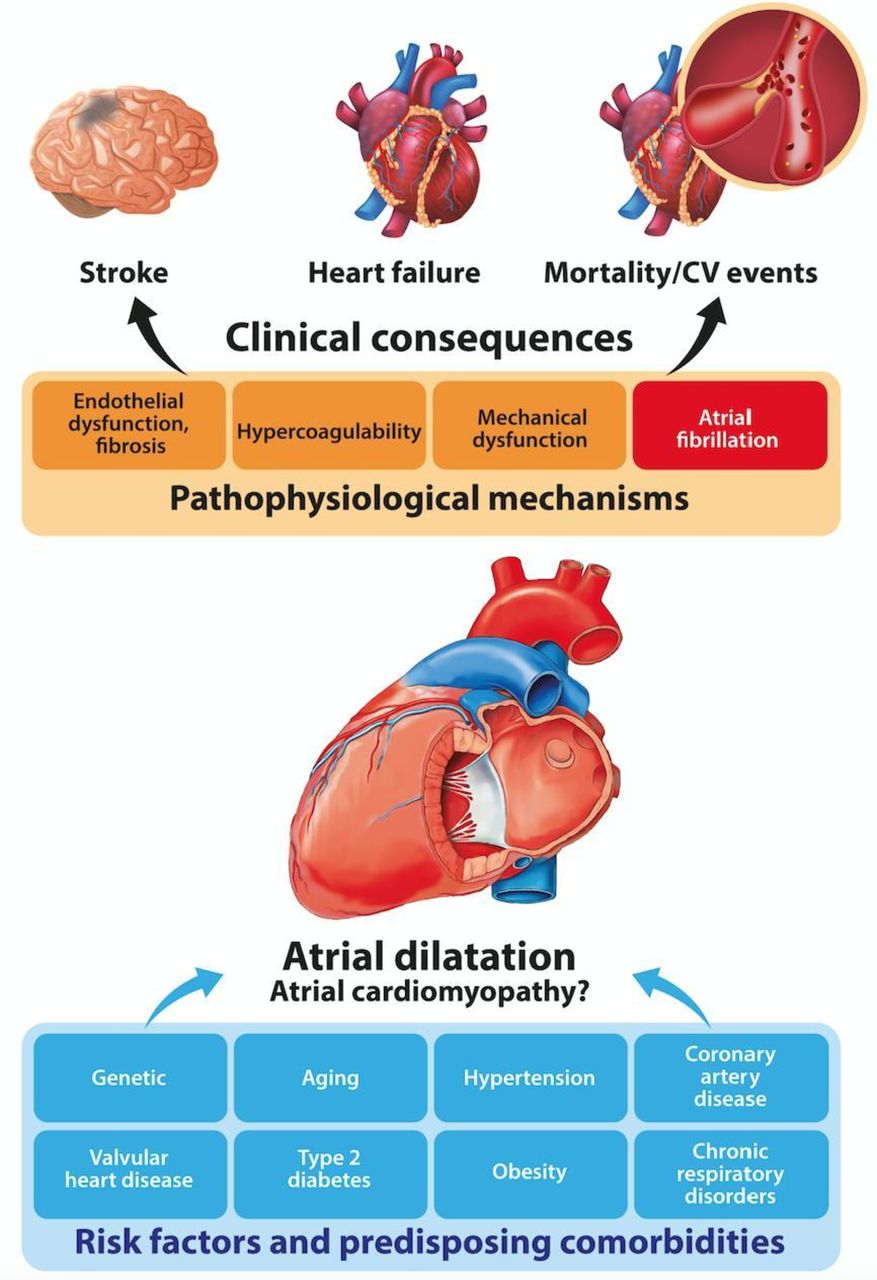
In the accompanying editorial, Polovina and colleagues2 review the role of the LA in cardiovascular homeostasis and offer insights into potential mechanisms of the association between LA size and adverse cardiovascular outcomes, as well as pointing out the strengths and limitations of this meta-analysis. They conclude: ‘the present meta-analysis emphasises the significance of LA dilatation as a prognostic biomarker for several important clinical outcomes, including stroke, incident HF and mortality in patients with and without AF. Whether the risk attributable to LA dilatation could be truly separated from the cumulative impact of left ventricular dysfunction and other risk factors remains uncertain’ (figure 2).

Risk factors and clinical consequences of left atrial dilatation.
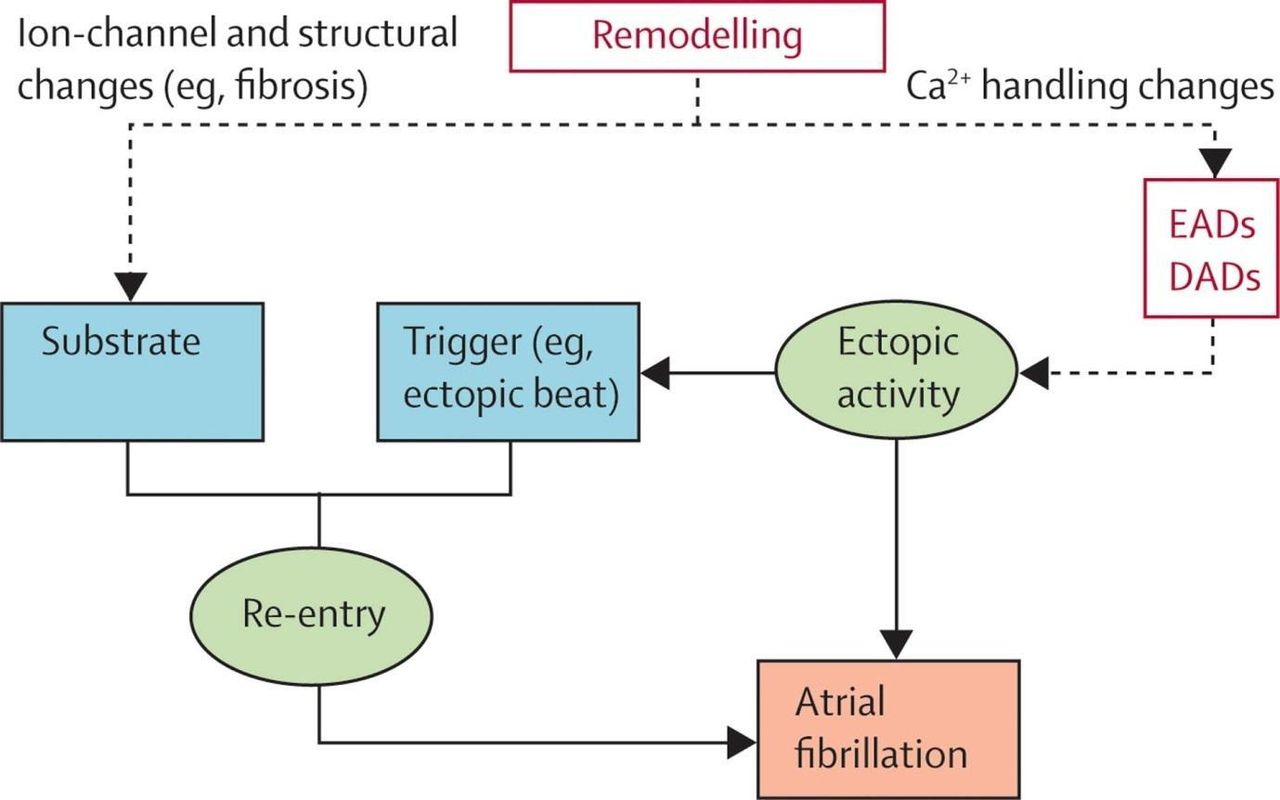
A review article on mechanisms of AF by Wijesurendra and Casadei3 provides further insight into the relationship between structural and electrophysiological changes in the LA and development of AF. The key concept is that AF is initiated and maintained by the interaction between a ‘trigger’ (eg, rapidly firing focus) and ‘substrate’ (eg, LA electrical and structural remodelling) (figure 3). Genetic factors increasingly are recognised as modulating AF risk with a 40% higher risk of incident AF in patients with an affected family member compared with those with no family history of AF. Identification of specific genes and pathways affecting these families ‘may allow new insights into AF pathophysiology, and potentially reveal new therapeutic targets’. In addition, ‘it has become increasingly recognised that AF is more than just an atrial disease, with documented associations with systemic inflammation, endothelial dysfunction, cardiometabolic disturbance and wider abnormalities in myocardial structure and function’

Key concepts underlying the induction and maintenance of atrial fibrillation (AF). AF can be maintained by either re-entrant or rapid and sustained ectopic activity. Development of re-entry depends on the action of a trigger (usually from an ectopic beat) acting on vulnerable substrate. In normal hearts, atrial electrical properties are less likely to support the maintenance of AF. Atrial remodelling creates a substrate for re-entrant AF, by altering ion channel function and/or inducing tissue fibrosis. Remodelling can also make ectopic activity more likely by producing changes in Ca2+ handling that promote both triggered activity and re-entry. DAD, delayed after depolarisation; EAD, early after depolarisation. Reproduced with permission from Dobrev D and Nattel S.9
In an exciting translational study using quantitative 18F-fluciclatide positron emission tomography (PET) to study disease mechanisms, Jenkins and colleagues4 showed that αvβ3 integrin activity is associated with plaque burden in human aortic atheroma and is higher in patients with recent myocardial infarction (figure 4). In an editorial, Tarkin and colleagues5 congratulate the authors on this detailed advanced imaging study and point out that ‘unlike conventional imaging targets in cardiovascular disease, PET imaging can provide unique markers of disease activity, such and inflammation and neoangiogenesis, which are central to the pathogenesis of disease’.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kinetic analysis of aortic 18F-fluciclatide uptake. Sagittal views of the thorax following kinetic analysis in two participants with (patient 1: A–E) and without (patient 2: F–H) aortic arch 18F-fluciclatide uptake. CT images confirm presence (A) or absence (F) of aortic arch calcification as a marker of established atheroma. Patlak slope (Ki) parametric images (B and G) identify focal uptake within the aortic arch in the region of atheroma (red arrow) localising to the vessel wall on the fused Patlak and CT images (C and H). Patlak modelling (D) confirms irreversible integrin binding within the region of aortic arch calcification (red arrow). Time activity curves within the same region (E) show a persistently high blood pool fraction, but uptake within atheroma that exceeds the blood pool fraction beyond 40 min (dashed line).
Other interesting articles in this issue of Heart include a study showing that the European Society of Cardiology (ESC) calculator for risk of sudden cardiac death in patients with hypertrophy cardiomyopathy (HCM) had a high negative predictive value and high accuracy in a cohort of 4288 Korean patients, although 1.1% of patients classified as low risk did have appropriate defibrillator therapy or sudden death.6 Maron and colleagues7 discuss the differences between the ESC and American College of Cardiology/American Heart Association (ACC/AHA) strategies for risk prediction in HCM patients and express the opinion that ‘the highly sensitive ACC/AHA major risk factor method of using ≥1 of the established individual risk factors considered major within the clinical profile of the patient with HCM, and associated with a greater measure of shared decision-making and opportunity for physician judgement, remains the preferred strategy for risk stratifying individual patients with HCM for primary prevention device therapy’.
The Education in Heart article in this issue8 reviews the rationale for specialised Heart Valve Clinics and offers practical advice on setting up and managing a Heart Valve Clinic. Figures and tables detail the roles of the essential team members, multidisciplinary interactions, types of testing needed and the approach to patient care and follow-up.
Footnotes
Contributors Commissioned article from journal EIC.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.