Article Text

Statistics from Altmetric.com
The recommendation in current guidelines that aortic valve replacement (AVR) be performed in adults with symptomatic severe aortic stenosis (AS) is based on solid evidence. However, it is unclear whether adults with asymptomatic severe AS also should be considered for elective AVR. This uncertainty is based on several considerations including the difficulty in recognising that symptoms are present and might be due to AS in older adults who often have multiple comorbidities, the concern that waiting for symptoms might be associated with irreversible cardiac changes, and the (although small) risk of sudden death. In addition, perhaps it makes sense to perform AVR before the patient is older and sicker, given the inevitable progression to symptoms once severe AS is present. On the other hand, both surgical and transcatheter AVR are associated with mortality and morbidity and the bioprosthetic valve is subject to deterioration, starting at the time of implantation.
In this issue of Heart, Nakatsuma and colleagues1 hypothesised that serum B-type natriuretic peptide (BNP) level would allow accurate risk stratification of adults with asymptomatic severe AS. In a large Japanese registry of adults with severe AS, data from the 387 patients with no symptoms and normal left ventricular systolic function showed that higher BNP levels were associated with a higher risk of adverse events (figure 1) with a 1 year event rate of only 2.1% in those with an BNP <100 pg/mL.

Kaplan -Meier curves for the primary outcome measure according to the baseline BNP levels. The primary outcome measure was defined as a composite of aortic valve-related death or HF hospitalisation. Patients were divided into four groups according to the baseline BNP levels (group 1: BNP<100 pg/mL, group 2: 100≤BNP<200 pg/mL, group 3: 200≤BNP<300 pg/mL and group 4: BNP>300 pg/mL). BNP, B-type natriuretic peptide; HF, heart failure.
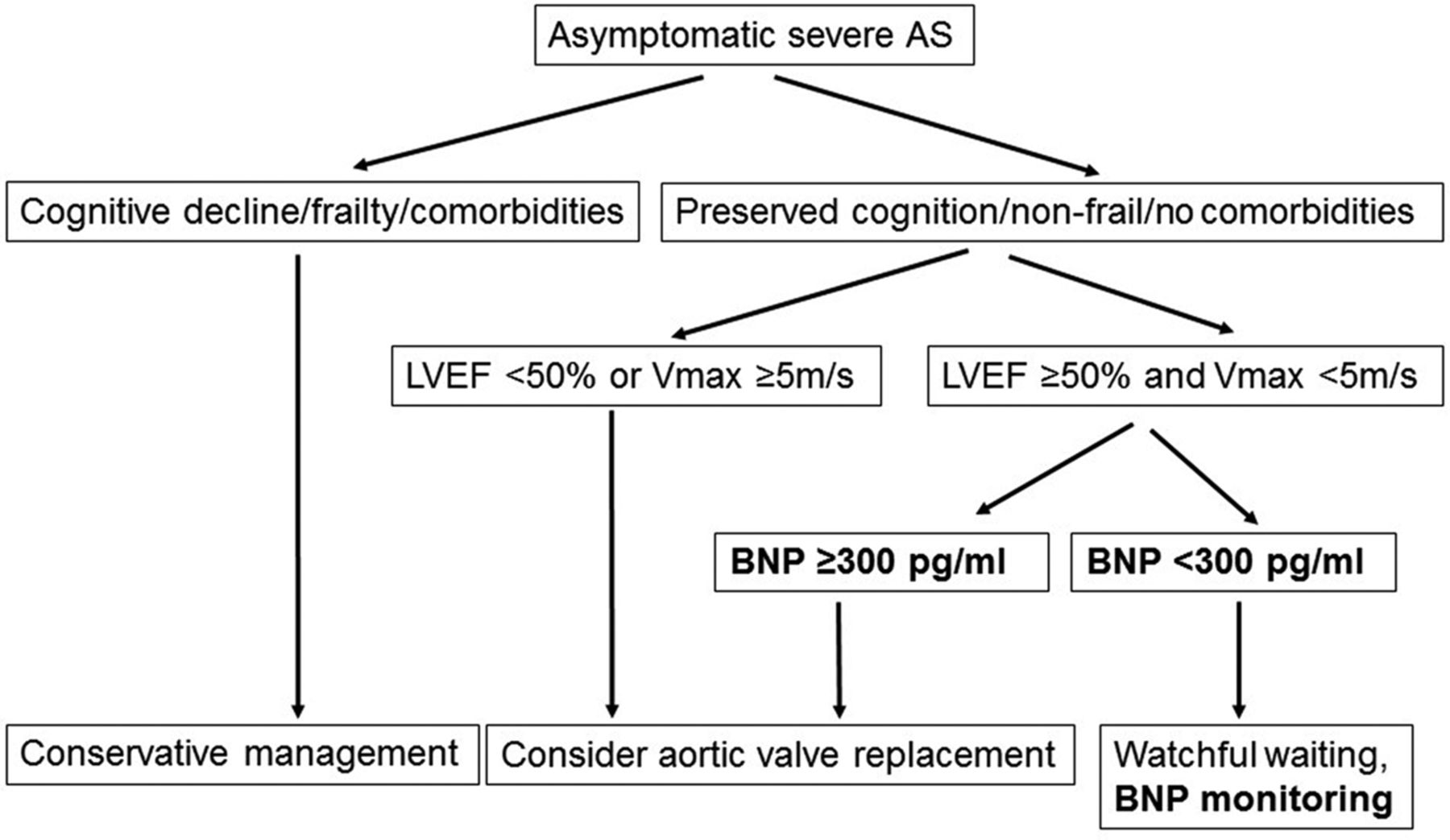
In the accompanying editorial, Martinez-Selles and Genis2 conclude that “While the role of biomarkers is promising, they must be thoroughly examined in clinical trials before entering into clinical practice. In the meantime, biomarker research is welcome to improve understanding of patients’ phenotypes and clinical progression.’ Although the evidence is not yet robust enough to support a strong recommendation, they suggest that clinicians may want to consider Integrating BNP levels into clinical decision making in adults with asymptomatic severe AS, particularly for identification of lower-risk patients who can be followed with periodic monitoring (figure 2).

A suggestion to incorporate B-type natriuretic peptide in the current guideline recommended approach in patients with asymptomatic severe aortic stenosis. AS, aortic stenosis; BNP, B-type natriuretic peptide; LVEF, left ventricular ejection fraction; Vmax, peak aortic jet velocity.
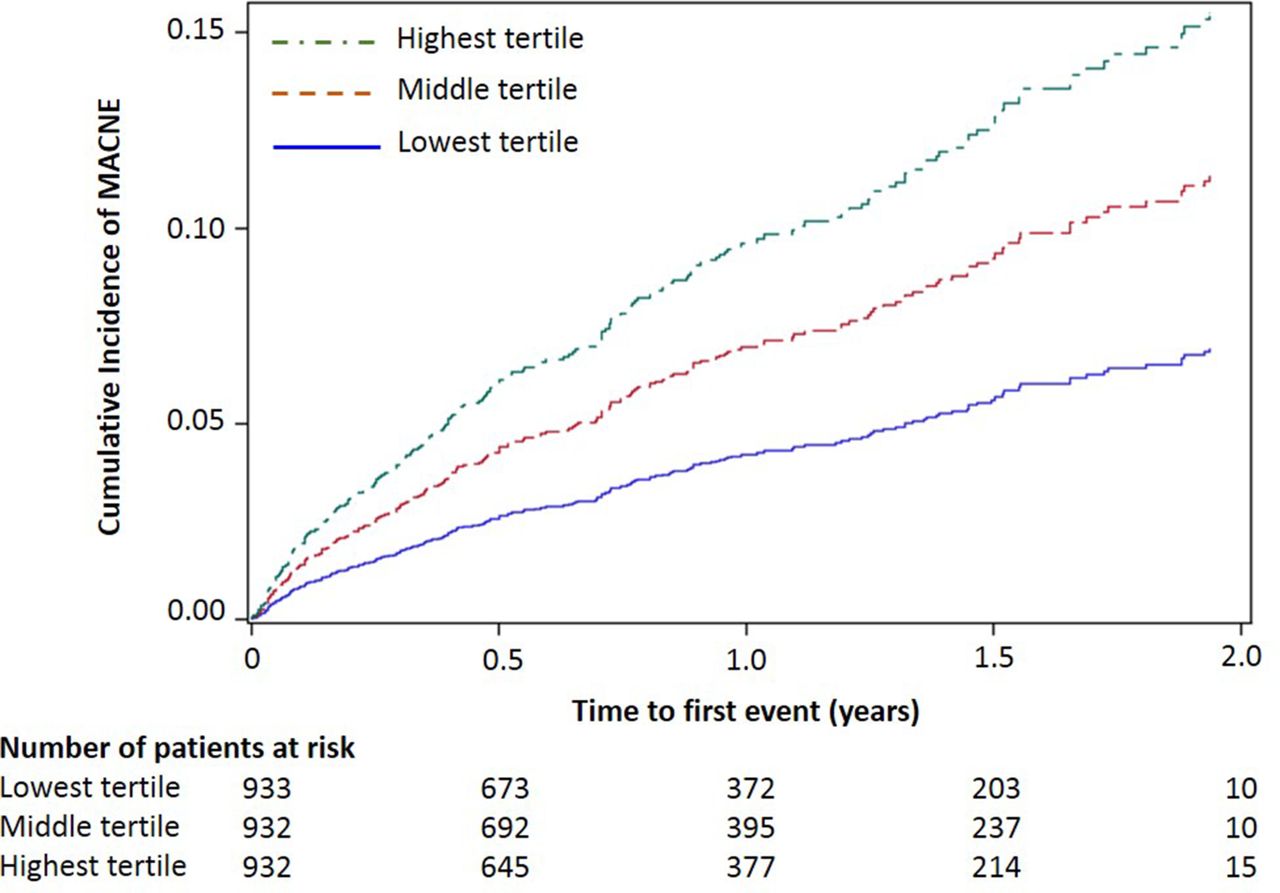
BNP levels also may be useful for risk stratification in adults with atrial fibrillation (AF). Inohara and colleagues3 analysed the association between BNP levels and clinical outcomes in 1282 patients with paroxysmal or persistent AF at baseline. Higher BNP levels were associated with both an increased likelihood of AF progression (adjusted OR, 1.11 for every 100 ng/mL; 95% CI 1.03 to 1.19) and major adverse cardiovascular or neurological events (adjusted HR, 1.11 for every doubling in BNP values; 95% CI 1.01 to 1.22) (figure 3).

Cumulative incidence curves for MACNE stratified by tertiles of BNP values. BNP, B-type natriuretic peptide; MACNE, major adverse cardiovascular or neurological event.
Given the prognostic value of BNP levels in adults with AF as demonstrated in this and other studies, Hijazi and Wallentin4 recommend that BNP be measured routinely in these patients. Further, they suggest that “The next step in the research on natriuretic peptides in AF should preferably focus on the usefulness of combinations of several biomarkers for an even better prognostication and on the utility of biomarker-based decision support to better individualise the therapy and improve outcomes in patients with AF.’
Worldwide, digoxin continues to be used in many patients with rheumatic heart disease (RHD) despite lack of data on the effect of therapy on clinical outcomes. In an effort to bridge this knowledge gap, Karthikeyan and colleagues5 found that digoxin use was significantly associated with higher 2 year mortality (OR 1.63, 95% CI 1.30 to 2.04, P<0.0001) and recurrent HF (OR 1.48, 95% CI 1.07 to 2.04, P=0.019) based on retrospective analysis of registry data that included over 3000 RHD patients. However, this effect was attenuated on propensity matching and a higher rate of adverse outcomes was only seen in patients in sinus rhythm without heart failure. In contrast, in those with both atrial fibrillation and heart failure, digoxin use was associated with lower mortality (OR 0.88, 95% CI 0.80 to 0.98, P=0.019).
These findings are put in context by Nascimento and Beaton6 who conclude “These data suggest a very narrow therapeutic benefit of digoxin among patients with RHD, with the most benefit in cases of combined HF and AF and potentially substantial harm when digoxin is prescribed for those with neither. However, strong recommendations for change in prescribing practices best await a randomised clinical trial, for which these data have set the stage. Until randomised trials, digoxin should be cautiously prescribed to patients with RHD, with an individualised approach and close clinical monitoring’ (figure 4).
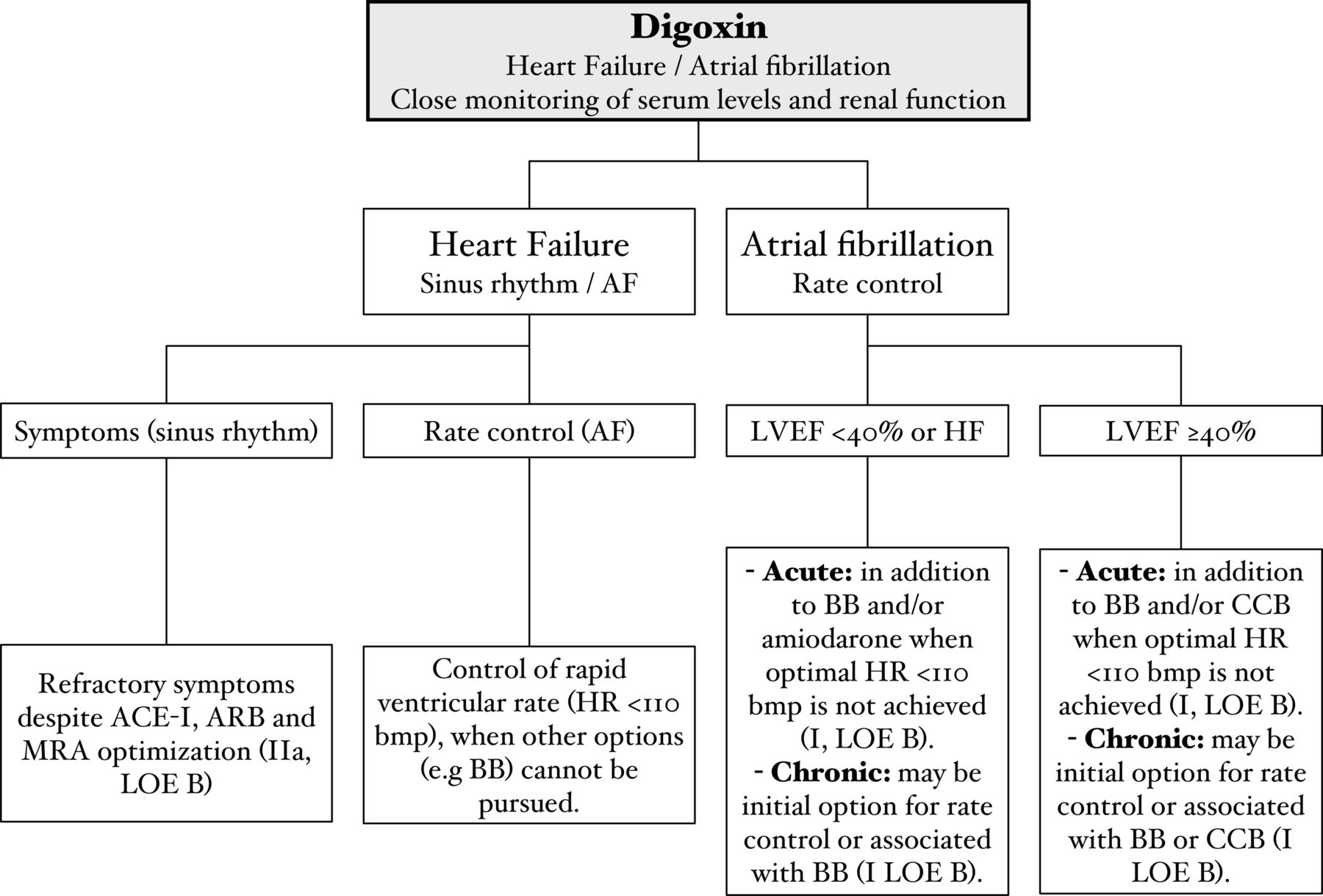
Flowchart with summary indications for digoxin prescription according to the European Society of Cardiology guidelines. ACE-I, ACE inhibitors; AF, atrial fibrillation; ARB, angiotensin receptor blockers; BB, beta-blockers; CCB, calcium channel blockers; HF, heart failure; HR, heart rate; LOE, level of evidence; LVEF, left ventricular ejection fraction; MRA, mineralocorticoid receptor antagonists. *Adapted from the European Society of Cardiology Guidelines.
The Education in Heart article7 in this issue reviews the epidemiology and clinical presentation of pulmonic valve stenosis in adults, summarises the expected disease course of treated and untreated disease, and discusses the indication for intervention in adults with pulmonary valve stenosis (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Classification of pulmonary valve stenosis. The pulmonary valve can be (A) a commissural or (B) unicommissural with prominent systolic doming of the cusps and an eccentric orifice. (C) Bicuspid pulmonary valve is shown with fused commissures. (D) Dysplastic pulmonary valve is severely thickened with deformed valve cusps.
The Image Challenge questions8 9 in this issue both show classic findings in unusual conditions. Definitely worth a few minutes to learn a little more cardiology in this interactive format!
Footnotes
Patient consent for publication Not required.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.