Article Text

Abstract
Objective To compare normothermic (35°C–36°C) versus hypothermic (28°C) cardiopulmonary bypass (CPB) in paediatric patients undergoing open heart surgery to test the hypothesis that normothermic CPB perfusion maintains the functional integrity of major organ systems leading to faster recovery.
Methods Two single-centre, randomised controlled trials (known as Thermic-1 and Thermic-2, respectively) were carried out to compare the effectiveness and acceptability of normothermic versus hypothermic CPB in children with congenital heart disease undergoing open heart surgery. In both studies, the co-primary clinical outcomes were duration of inotropic support, intubation time and postoperative hospital stay.
Results In total, 200 participants were recruited; 59 to the Thermic-1 study and 141 to the Thermic-2 study. 98 patients received normothermic CPB and 102 patients received hypothermic CPB. There were no significant differences between the treatment groups for any of the co-primary outcomes: inotrope duration HR=1.01, 95% CI (0.72 to 1.41); intubation time HR=1.14, 95% CI (0.86 to 1.51); postoperative hospital stay HR=1.06, 95% CI (0.80 to 1.40). Differences favouring normothermia were found in urea nitrogen at 2 days geometric mean ratio (GMR)=0.86 95% CI (0.77 to 0.97); serum creatinine at 3 days GMR=0.89, 95% CI (0.81 to 0.98); urinary albumin at 48 hours GMR=0.32, 95% CI (0.14 to 0.74) and neutrophil gelatinase-associated lipocalin at 4 hours GMR=0.47, 95% CI (0.22 to 1.02), but not at other postoperative time points.
Conclusions Normothermic CPB is as safe and effective as hypothermic CPB and can be routinely adopted as a perfusion strategy in low-risk infants and children undergoing open heart surgery.
Trial registration number ISRCTN93129502.
- Congenital Heart Disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Whole body cooling is an integral part of congenital cardiac surgery, with most procedures being conducted at 28°C.1 The main rationale for body cooling is to protect the brain, kidneys and heart from ischaemic injury, by reducing the metabolic rate and decreasing oxygen consumption.2 In recent years, there has been an increasing interest in normothermic cardiopulmonary bypass (CPB) during adult cardiac surgery. The concept that normothermic systemic perfusion may confer advantages over hypothermic regimes arose from adult clinical experience in which an absence of shivering, haemodynamic stability, mimimal inotropes and early extubation was observed when patients were not cooled. This led several investigators to study the effects of systemic hypothermia and normothermic perfusion on cellular and organ function.3–6 CPB perfusion temperature strategies and their effects on the function of several organs are largely the result of work carried out on adult humans and the conclusions cannot necessarily be applied directly to infants or children. Having demonstrated that in infants and children undergoing cardiac surgery, normothermic CPB was associated with reduced oxidative stress and similar myocardial reperfusion, renal injury and inflammatory response compared with hypothermic CPB,7 8 we hypothesised that maintaining the body at 35°C–37°C (normothermia) rather than cooling to 28°C (hypothermia) during surgery could translate into better clinical outcomes. We report the results of two trials referred to as Thermic-1 and Thermic-2, respectively, designed to compare the clinical effectiveness of normothermic versus hypothermic CPB for the repair of common congenital cardiac pathologies.
Methods
Trial design
Our study includes the Thermic-1 and Thermic-2 trials, which are single-centre, parallel-group open randomised controlled trials (RCTs). Participants were randomly allocated to receive either hypothermic or normothermic CPB in a 1:1 ratio. The Thermic-2 trial is registered (ISRCTN93129502) and details of the trial design are reported elsewhere.9
Participants
Patients (aged ≤18 years) having scheduled surgery to repair a congenital heart defect using CPB were eligible to participate. Patients admitted for an emergency operation and those requiring deep hypothermic circulatory arrest were excluded. Parents/guardians (if aged under 16 years) provided written informed consent, and children aged 11–15 years provided written assent.
Both studies were conducted at the Bristol Royal Hospital for Children, a regional congenital cardiac surgery centre in the UK. Thermic-1 recruited patients between 2002 and 2004, and Thermic-2 between 2012 and 2014. All paediatric cardiac surgeons participated in Thermic-2.
Interventions
Eligible patients were randomised to receive either normothermic or hypothermic CPB. CPB and anaesthetic management adhered strictly to a locally agreed protocol, details of which are reported elsewhere.7 9 In the hypothermic group, the CPB temperature was targeted to decrease until the nasopharyngeal body temperature had lowered to 28⁰C and in the normothermic group the CPB temperature was targeted to maintain the nasopharyngeal temperature at 35°C–36°C. Rewarming commenced after completion of the anatomical correction and only took place in the normothermic group if the body temperature dropped below 36°C. In both groups, CPB was discontinued only after the participant was fully rewarmed to above 36⁰C. The CPB flow rate was kept at 2.6–2.8 L/min/m2 and cold blood (4°C–6°C) cardioplegia (4:1 dilution blood/St Thomas' no. I crystalloid cardioplegia) was used for myocardial preservation in all patients.7 8
Outcomes
The co-primary end points were: i) duration of inotropic support, ii) intubation time and iii) postoperative hospital stay (from date of surgery to discharge from cardiac ward). Inotropic support was standardised; dopamine and milrinone were started in the operating room before weaning from CPB. Epinephrine was used if a low cardiac output state persisted. All the inotropic support drugs were weaned in the paediatric intensive care unit (PICU) according to the unit protocol. Secondary outcomes were in-hospital mortality and morbidity; blood loss and transfusion requirements; postoperative echocardiographic findings; near-infrared spectroscopy (NIRS) during CPB, renal function measured by urea nitrogen, serum creatinine, urinary albumin, urinary creatinine, retinal binding protein (RBP), N-acetyl-β-glucosaminidase (NAG) and neutrophil gelatinase-associated lipocalin (NGAL); cerebral function measured by glial fibrillar acidic protein (GFAP); neuropsychological development, assessed using the NEPSY-II psychometric tool (valid for participants aged ≥3 years and <17 years only). Unexpected serious adverse events (SAEs) were coded using the Medical Dictionary for Regulatory Activities (V.14.1; McLean, VA, USA).
Renal function was measured from serial blood and urine samples taken preoperatively, at cross clamp removal and 4, 24 and 48 hours thereafter. Cerebral function was assessed preoperatively, at cross clamp removal and 30 min and 2, 6, 24 and 48 hours thereafter. NEPSY-II was assessed preoperatively and at 3 and 12 months postoperatively.
There were no changes to the outcomes during Thermic-1. Several secondary outcomes were added to the Thermic-2 protocol after the start of the study: RBP, NAG and NGAL markers of renal function (collected for a subset of 60 patients not having isolated atrial septal defect surgery); and NIRS. In addition, the marker of brain damage was changed from protein S100B to GFAP, to give a more accurate measure of cerebral function.9 10
Sample size
Full details of the power calculations are reported elsewhere.11 Briefly, a sample size of 200 patients (100 per group) was required to detect reductions of: 1 day or greater in length of postoperative stay, 3 hours in ventilation time and 4.7 hours in inotropic support with 90% power, assuming a 5% level of statistical significance (two-tailed).
Randomisation
Randomisation was stratified by age (≤1 month, 1–12 months and >12 months). Allocations were computer generated using block randomisation with varying block sizes by a statistician independent of the study team. A password-protected database concealed allocations until data had been entered to confirm identity and eligibility. Randomisation, which took place as close to the start of surgery as possible, was carried out by the study coordinator who placed the allocation details in an opaque sealed envelope before handing it to the perfusion team.
Blinding
Participants and their parents/guardians were blinded to the treatment allocation. Staff involved in the operation were unblinded but the allocation was not disclosed until after the start of the operation. Staff caring for participants postoperatively were not actively informed of the participant’s allocation, although they could have become unblinded as they have access to the anaesthetic and perfusion charts which must be stored in the medical notes.
Echocardiographic findings were interpreted by cardiologists blinded to the treatment allocation. Laboratory analyses and the NEPSY-II test administration were carried out by blinded researchers. All other outcomes were ascertained directly from medical notes, PICU charts and electronic hospital records.11
Statistical methods
Analyses were based on a prespecified statistical analysis plan (SAP) and performed on an intention-to-treat (ITT) basis. Outcomes were compared using logistic regression (binary outcomes), linear regression (continuous outcomes), Cox proportional hazards regression with appropriate censoring (time-to-event outcomes) or mixed-effects regression (continuous longitudinal outcomes); see online supplementary material for further details. All analyses used the hypothermic group as the reference group and were adjusted for trial phase (Thermic-2 vs Thermic-1) and age (>12 vs ≤12 months). Results are reported as effect sizes with 95% CIs. Serial measurements taken as part of routine care (eg, blood gases) are described and frequencies of adverse events are tabulated. Prespecified subgroup analyses by trial phase (Thermic-1 vs Thermic-2) were performed by adding an interaction term to the models. Analyses specified in the SAP but not in the study protocol were a) sensitivity analyses: i) excluding protocol deviations (all deviations, and only those deemed major), ii) reanalysing inotropic data including only dopamine, the only inotrope collected in both trial phases and b), analyses of each component of the primary outcome using instrumental variable (IV) techniques to estimate the unbiased effect of CPB temperature, with randomised allocation as the instrument (see online supplementary material). Analyses were performed in Stata V.14.0 (StataCorp, College Station, Texas, USA).
Supplementary file 1
Results
Recruitment
Between August 2002 and February 2004, 59 patients consented to participate in the Thermic-1 trial and were randomised (screening data unavailable). Between January 2012 and October 2014, 449 patients were screened for inclusion in the Thermic-2 trial, 49 of whom were ineligible. In total, 231 families of the eligible patients were approached and 141 consented and their child was randomised (61%). Combined across both trial phases, 98 participants were allocated to the normothermic group and 102 to the hypothermic group (figure 1).

Flow of participants. *One patient was withdrawn by the clinician postrandomisation but presurgery. As the patient was happy for data collection to continue, they have remained in the analysis population. ASD, atrial septal defect; PIL, patient information leaflet.
The primary analysis includes all randomised participants. There were 10 treatment cross-overs, 8 in the hypothermic group and 2 in the normothermic group (see online supplementary table S1). Thermic-1 participants were followed up to hospital discharge only. Thermic-2 participants were followed up for 12 months. Safety data were collected for Thermic-2 participants to 12 months.
Baseline data
The median age was 3.4 years (range 6 days–17.9 years); participants in Thermic-1 were, on average, older than in Thermic-2 (table 1 and online supplementary table S2). Overall, 95/200 (48%) were male. Most participants scored a risk-adjusted congenital heart surgery (RACHS) score of 2 or 3 (163/200; 82%). A significant proportion of participants had undergone cardiac surgery previously (44/200; 22%). Overall, characteristics were generally well balanced across the groups.
Patient demography
Operative details
All measures of operative duration were longer in the normothermic group than the hypothermic group by approximately 10 min (table 2 and online supplementary table S3). These differences were reflected in Thermic-2, but not in Thermic-1. Median temperatures were similar to pre-CPB. During CPB, the median temperature in the normothermic group was 34.8°C vs 28.6°C in the hypothermic group, and at cross-clamp removal 36.1°C vs 35.0°C, respectively. By the end of CPB, temperatures had reverted to similar levels in the two groups. All other characteristics were similar; haemodynamic instability (8/140; 6%), the need for cardioversion (3/187; 2%) and ischaemic changes when coming off CPB (2/113; 2%) were rare. All received inotropes when coming off CPB.
Intraoperative characteristics
Primary outcome
Treatment estimates for the three co-primary outcomes are shown in figure 2. The duration of inotropic support was similar in the two groups (median 23 hours (IQR 16–39) in the normothermic group vs 21 hours (IQR 14–44) in the hypothermic group) (see online supplementary figure S1 and table S4). Intubation time was shorter in the normothermic group (median 10.6 hours (IQR 5.9–25.3) vs 16.4 hours (IQR 6.1–26.6)), although this difference was not statistically significant (see online supplementary figure S2). The median postoperative hospital stay was 6.0 days in both groups (IQR 5.0–7.0, online supplementary figure S3). Maximum inotropic score and vasoactive-inotropic score12 were also similar (see online supplementary table S5, figure 3).
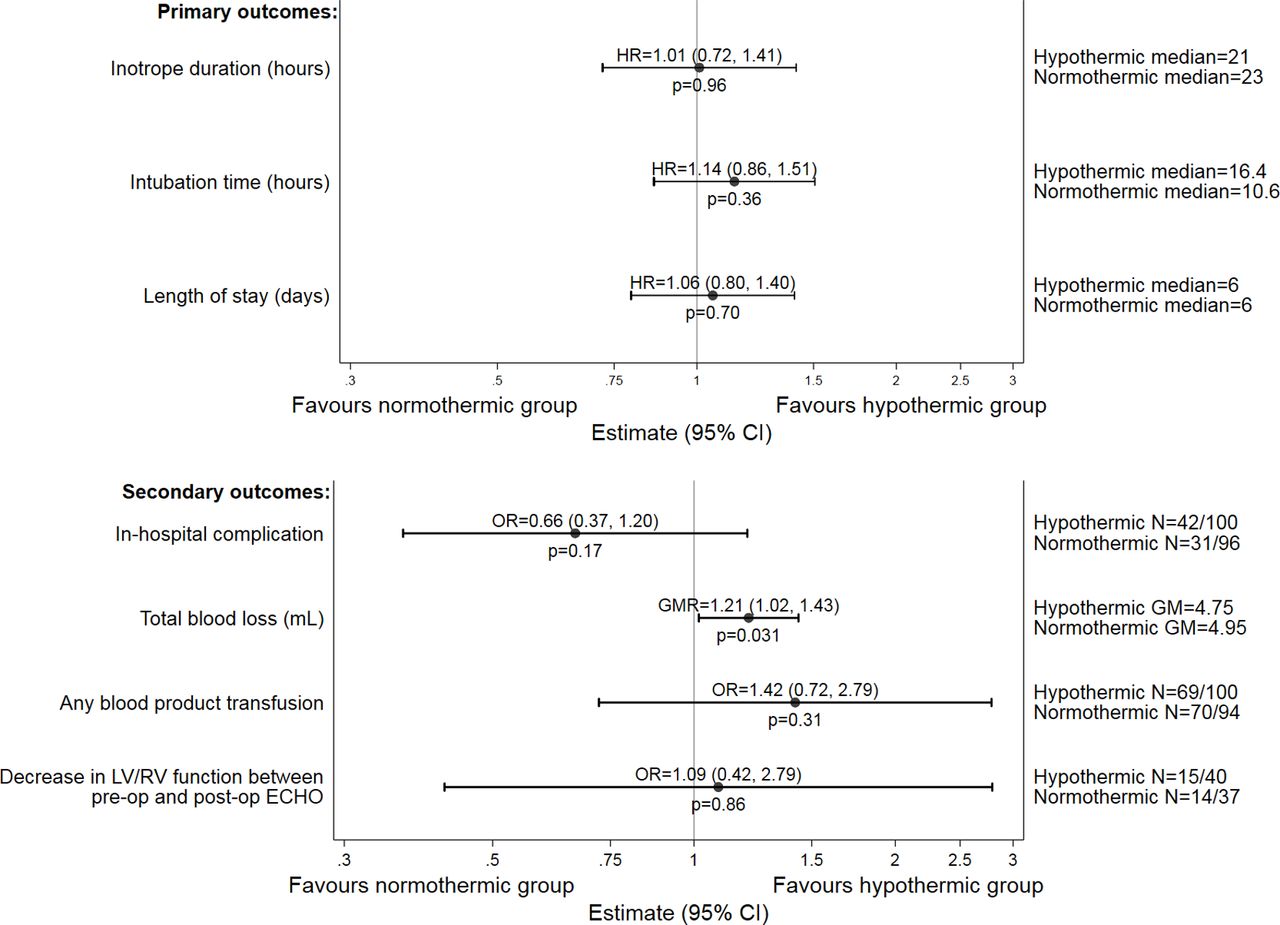
Primary and secondary outcomes. Duration of inotropic support was not collected in Thermic-1, and so the model only includes data from Thermic-2. It was not possible to adjust the inotrope duration model for age group (proportional hazards assumption was violated), and therefore the model is stratified by age group. Kaplan-Meier plots for each primary outcome are given in online supplementary figures S1-S3, further details of inotrope types are given in online supplementary table S4. Further details of the secondary outcomes are given in online supplementary table S5-S6. GM, geometric mean; GMR, geometric mean ratio; LV, left ventricular; RV, right ventricular.
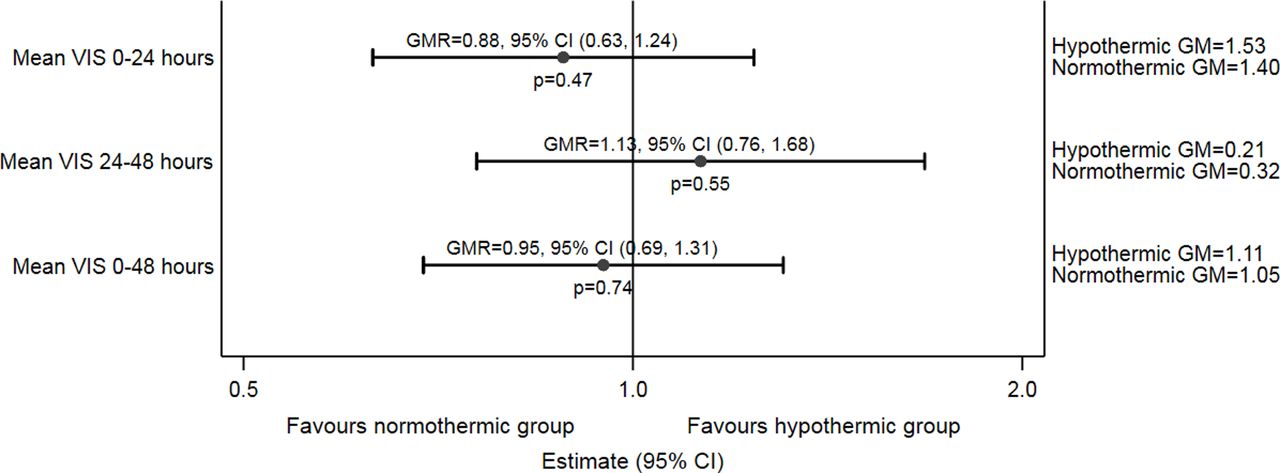
Comparison of mean VIS between normothermic and hypothermic groups. GM, geometric mean; GMR, geometric mean ratio; VIS, vasoactive-inotropic score.
Secondary outcomes
There were fewer postoperative complications in the normothermic group (31/96; 32% vs 42/100; 42%), although this difference was not statistically significant, figure 2). This difference was primarily due to fewer pulmonary complications and pericardial effusions (see online supplementary table S6). Total blood loss was, on average, 21% higher in the normothermic group (median 145.0 mL (IQR 100.0–200.0) vs 117.5 mL (IQR 90.0–175.0), figure 2), but this did not translate into a significant difference in rates of postoperative blood product transfusions (70/94; 74% normothermic group vs 69/100; 69%) and haemoglobin levels were similar (see online supplementary table S6, figures S8 and S15). Similar proportions of patients had a decrease in left/right ventricular function after surgery (14/37; 38% vs 15/40; 38%, see online supplementary table S7). Profiles over time of serial blood gases measurements and tests carried out as part of usual care were similar between the groups (see online supplementary figures S4 to S27). There was evidence of a treatment difference for NIRS readings (see online supplementary figure S28) with lower values in the normothermic group (mean difference=3.63, 95% CI (−6.91 to −0.36); p=0.033).
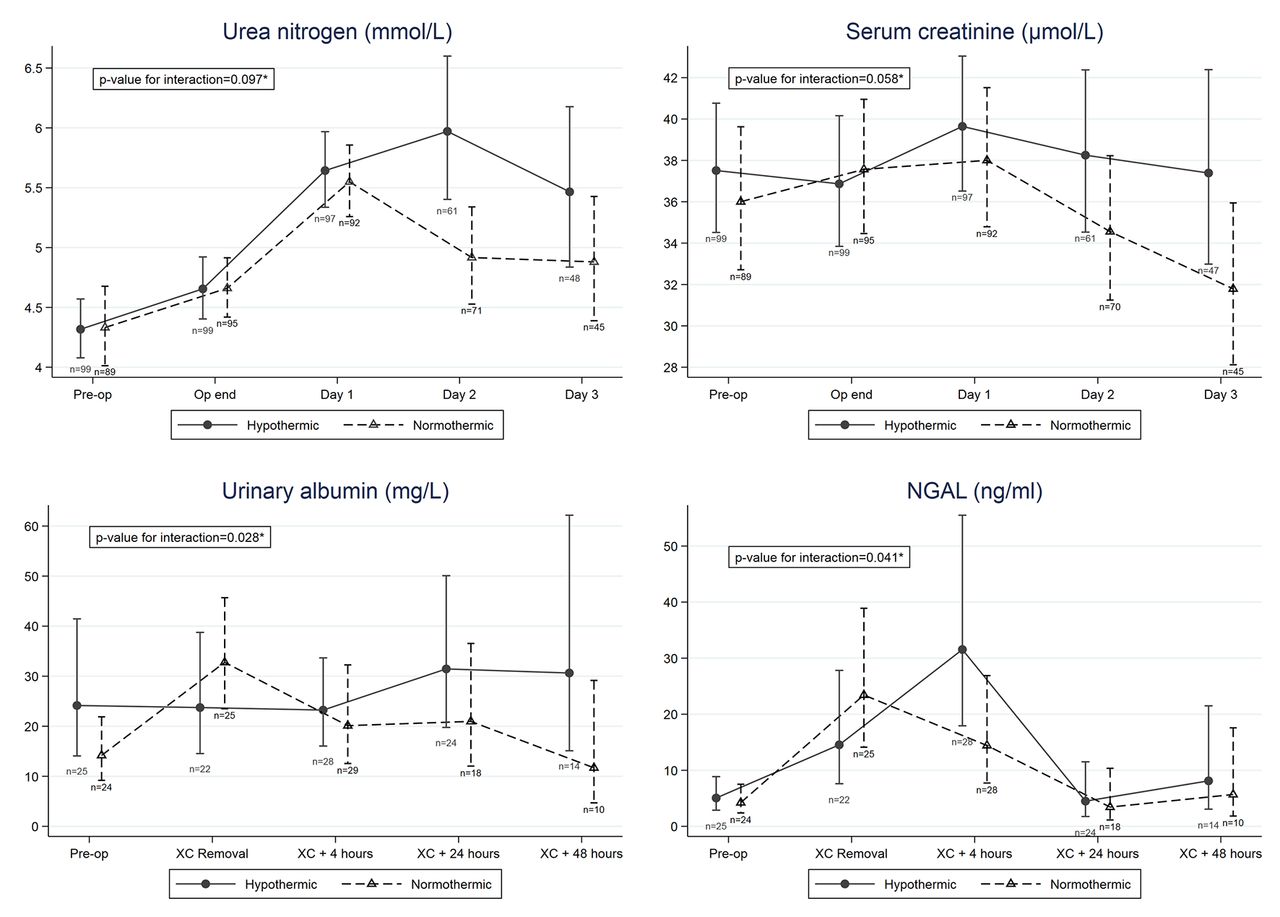
Renal function measured from blood and urine samples are given in figure 4, online supplementary figures S29 to S31 and tables S8 and S9. Significant treatment time interactions (at 10% level) were found for urea nitrogen, serum creatinine, urinary albumin and NGAL, driven by treatment differences (all favouring the normothermic group) at one time point, namely a difference in urea nitrogen on day 2, serum creatinine on day 3, urinary albumin 48 hours after cross-clamp and NGAL 4 hours after cross-clamp. For urinary creatinine, RBP and NAG, no statistically significant differences between the groups were found.
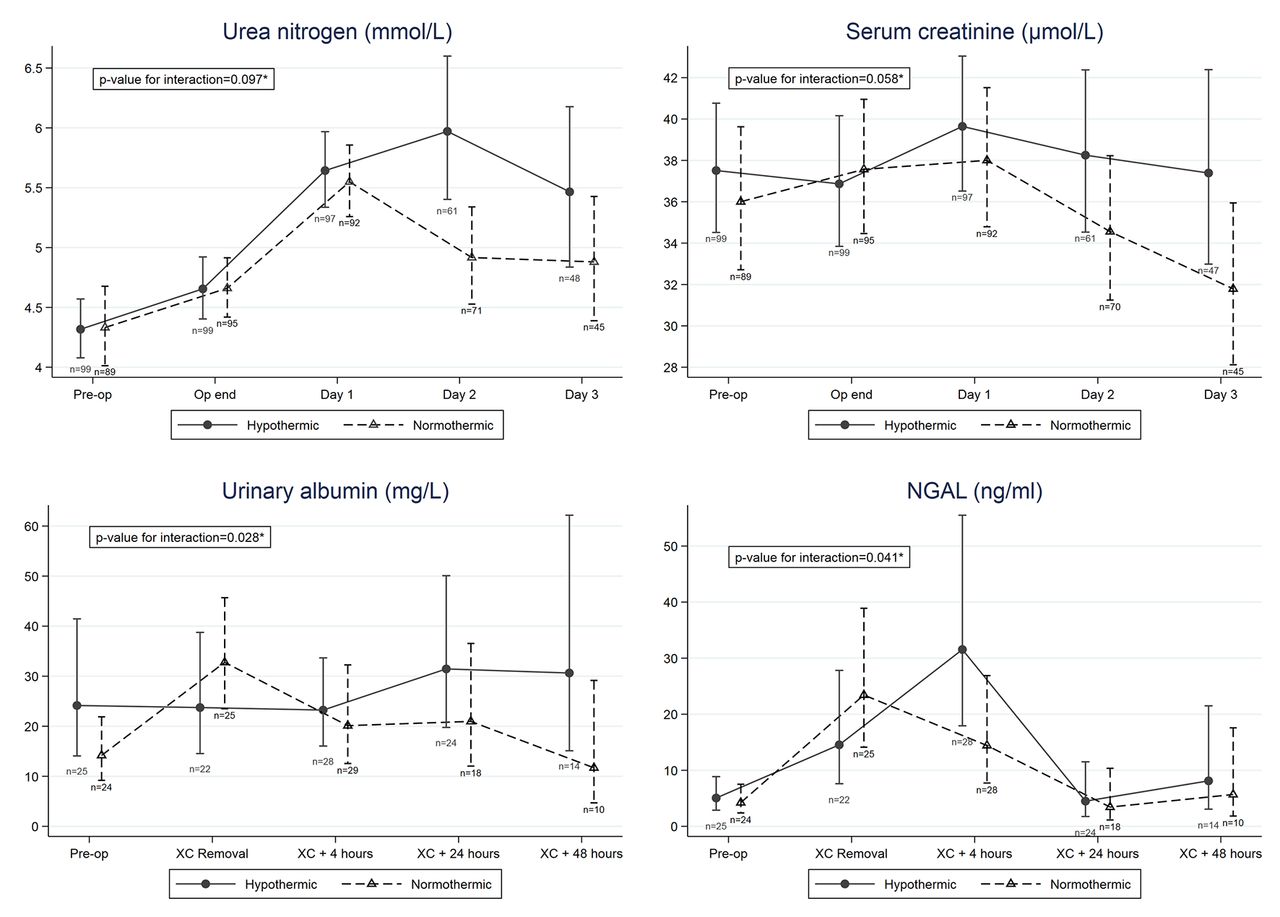
Renal function. Further details are given in online supplementary table S8 and S9. NGAL, neutrophil gelatinase-associated lipocalin; XC, cross-clamp.
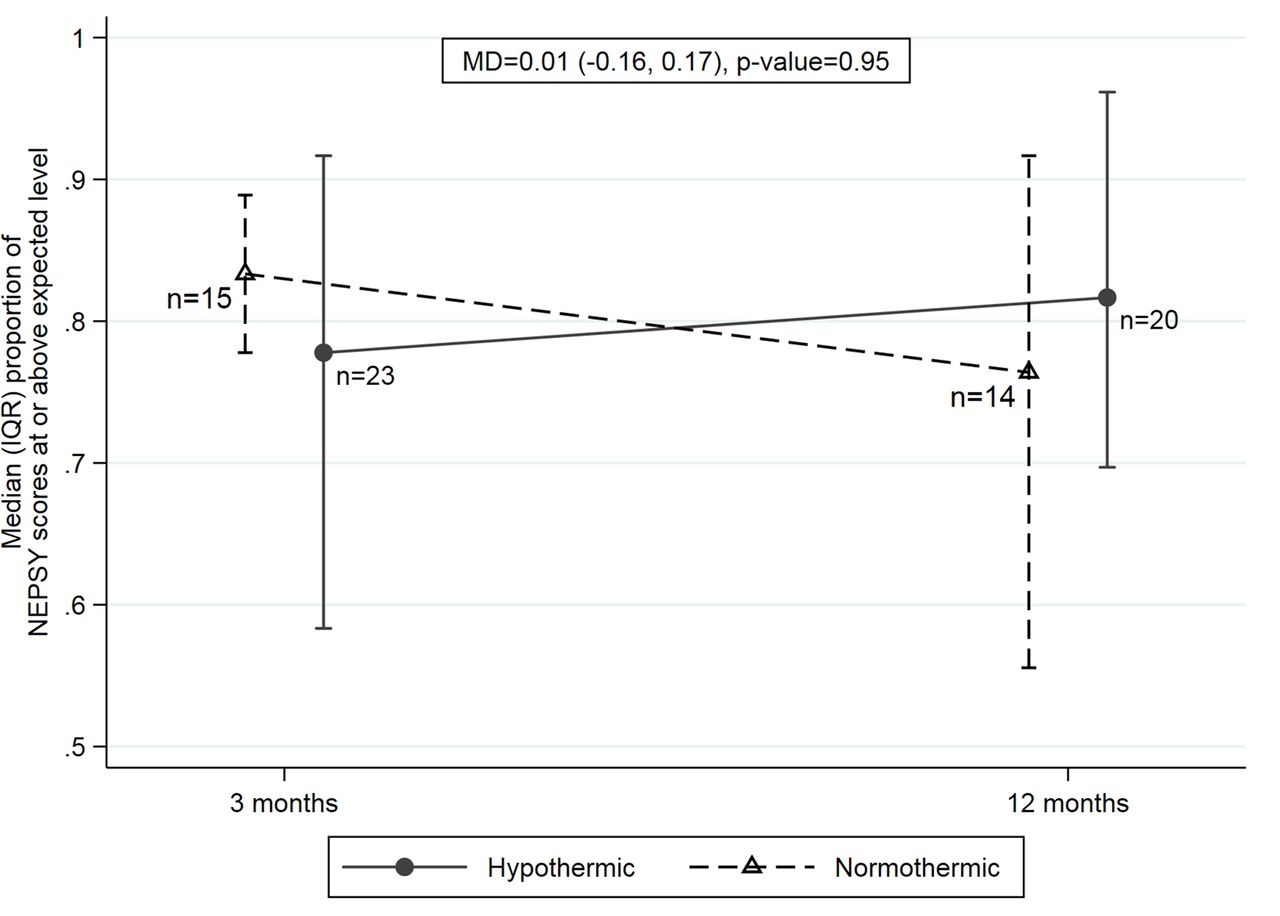
Cerebral function measured by GFAP is summarised in figure 5 and online supplementary table S10. There were no statistically significant differences between the groups, although the direction of effects suggested slightly higher GFAP values in the normothermic group. Neuropsychological developmental assessment (NEPSY-II) data are shown in figure 6 and online supplementary table S11. There were no clear differences between the groups for this outcome.
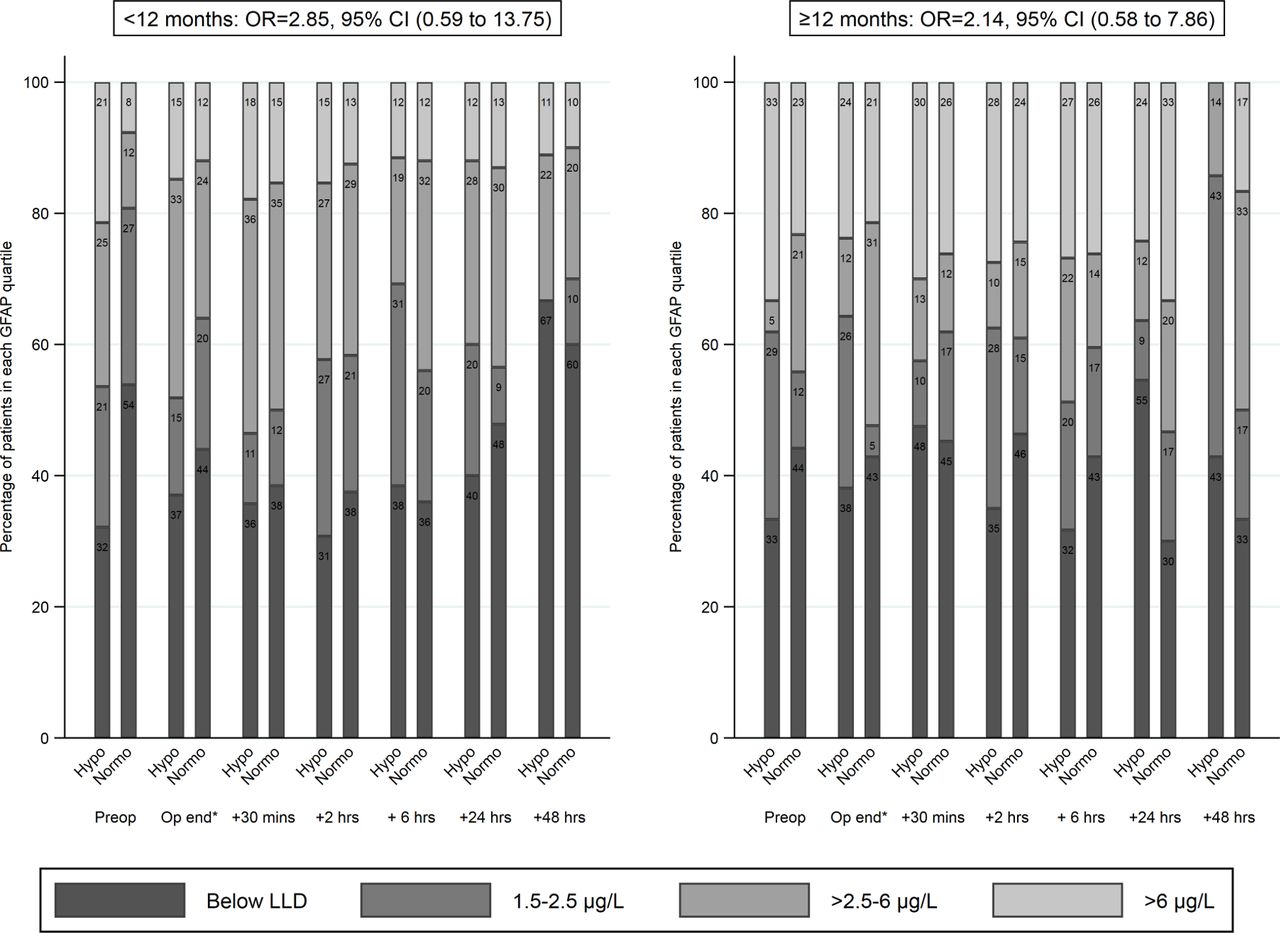
Cerebral function—GFAP. GFAP could not be modelled as continuous data due to the large amount of reading that were below the lower limit of detection (1.5 µg/L). Therefore, data were categorised into quartiles and modelled using mixed-effects ordinal logistic regression. The model was stratified by age to ensure the proportional odds assumption was met. Further details are given in online supplementary table S10 . *Operation end was defined as cross-clamp removal. GFAP, glial fibrillary acidic protein; LLD, lower limit of detection.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Neuropsychological development. The figure represents the median proportion of individual NEPSY domains where the child scored at or above the expected level (note the number of domains scored varied according to the age of the child). This proportion was analysed using a mixed-effects linear model. Three patients (all normothermic at 3 months) were excluded from the above analysis as <50% of the relevant NEPSY domain scores had been completed. Details of individual NEPSY scores are given in online supplementary table S11. MD, mean difference; NEPSY, NEPSY second edition psychometric tool.
Ancillary analyses
Sensitivity analyses excluding protocol deviations and considering only dopamine usage did not substantially alter the treatment estimates or change conclusions (see online supplementary tables S12 and 13, supplementary figure S32). Subgroup analyses by trial phase (see online supplementary figure S33) suggested a significant difference in treatment estimate between the two phases for length of stay, p value for interaction=0.079. Within Thermic-1 the estimated HR was 1.57, 95% CI (0.93 to 2.64), suggesting earlier discharge in normothermic group, compared with HR 0.90, 95% CI (0.65 to 1.26) within Thermic-2. Treatment estimates were similar for other outcomes between Thermic-1 and Thermic-2. The IV estimates of the effect of actual CPB temperature on outcome (rather than the effect of the ‘intended’ temperature as assessed in the primary ITT analyses) for each element of the primary outcome are given in online supplementary table 14. The IV analyses produced similar findings to the ITT analyses.
Follow-up to 1 year (Thermic-2 only)
In the normothermic group, 25/70 (36%) patients experienced an adverse event listed in the study protocol as anticipated after cardiac surgery compared with 29/71 (41%) hypothermic patients. A total of 127 SAEs (ie, prolonged the initial hospital stay or resulted in a further stay in hospital) were reported in 56 participants (66 events in 27/69 (39%) patients in the normothermic group vs 61 events in 29/71 (41%) patients in the hypothermic group, online supplementary table 15). There were no deaths within 1 year.
Discussion
The combined results of the Thermic trials suggest normothermic CPB is safe with no evidence of a clinical advantage in cooling the body of low-risk infants and children undergoing open heart surgery. Inotrope duration, intubation time and postoperative stay were similar in the two groups, a conclusion supported by the IV analysis. These results are clinically important given that moderate hypothermia (26°C–30⁰C) is still widely used in this patient population. Practise among congenital cardiac surgeons in relation to systemic cooling is variable, with a significant proportion still cooling the child’s body to 26°C–30°C.1 Our results are consistent with Pochelet et al (RCT, n=47), who demonstrated that normothermic CPB protocols are reproducible and safe.13
Hypothermic CPB is still considered the most effective strategy for protecting the brain during surgery, aiming for a low metabolic state and providing protection in case of increased blood return and the subsequent reduction in bypass flow or perfusion failure. However, these problems are extremely rare. There is no cardiac surgical evidence from newborns with asphyxial encephalopathy that moderate hypothermia (34°C) protects the brain, and there is no advantage from further cooling these neonates.14 15 We found no significant difference in cerebral function between the groups (as measured by GFAP levels), and the neuropsychological outcomes were also similar, suggesting that a normothermic strategy safely protects the brain. Previous neurological evaluations also failed to demonstrate differences between the hypothermic and normothermic groups in terms of verbal, performance and full-scale intellectual neuropsychological development.13
Significant differences in renal function, in favour of normothermic CPB, were observed across several markers of renal damage. This is important as acute kidney injury is a common postoperative complication and independently associated with adverse outcomes including mortality. The higher NGAL levels 4 hours postoperatively in the hypothermic group are indicative of renal tubular injury that can be exacerbated by the cooling and rewarming process. This phenomenon has been previously shown in adult cardiac surgery.16 We also found a trend towards lower levels of NAG and albumin (−14% and −37%, respectively) when expressed as a urinary creatinine ratio in Thermic-1.8
The only significant difference in favour of the hypothermic group was reduced blood loss, but this did not lead to a significantly lower transfusion rate and postoperative haemoglobin levels were similar in the two groups. Also, there was a tendency towards higher NIRS readings during CPB in the hypothermic group, but this did not correlate with other outcomes. Evidence suggests that NIRS in isolation is not very sensitive in predicting low cardiac output and neurological dysfunction after paediatric cardiac surgery and should be used alongside other haemodynamic and clinical metrics.17 18
The longer median cross-clamp time in the normothermic group was unexpected but is likely due to the higher proportion of more complex procedures in Thermic-2 (44% with RACHS score of 3 or 4 in the normothermic group vs 28% in the hypothermic group).
Strengths and limitations
Strengths include the inclusive eligibility criteria and minimisation of bias through concealed allocation. Within both trials the blood and urinary samples were analysed in a single hospital laboratory, thereby avoiding interlaboratory variability, and laboratory personnel were blinded to the group allocation.
With respect to limitations, participants were recruited from a single centre, limiting the generalisability of the findings. The two trials were carried out 10 years apart and there were differences between the two cohorts; participants in Thermic-1 were younger and bypass and cross-clamp times were shorter than in Thermic-2. There were also imbalances in preoperative characteristics between the two groups in Thermic-1, which may account for the greater difference in length of stay between the groups observed in Thermic-1. Some outcomes were collected in Thermic-2 only, reducing the power to detect differences between the two groups for these outcomes. The lack of blinding of the operating room team and the potential for staff caring for participants postoperatively to determine the allocation from the medical records represents a further weakness. Finally, very few neonates were recruited. Although there is observational evidence that normothermic CPB is safe and effective in neonates undergoing cardiac surgery,19 20 RCT evidence in this subgroup is lacking.
Conclusion
Normothermic CPB is safe and can be adopted as a perfusion strategy in low-risk infants and children undergoing open heart surgery.
Key messages
What is already known on this subject?
In infants and children undergoing open heart surgery, normothermic cardiopulmonary bypass (CPB) is associated with reduced oxidative stress and similar myocardial reperfusion, renal injury and inflammatory response compared with hypothermic CPB.
What might this study add?
We have demonstrated that in low-risk and medium-risk patients undergoing open heart surgery keeping the body warm (35°C−36°C) during CPB is clinically safe and effective.
Duration of inotropes, intubation and length of stay were similar with a normothermic strategy as with a hypothermic strategy.
How might this impact on clinical practice?
Normothermic CPB is safe and can be adopted as a perfusion strategy in low-risk to medium-risk infants and children undergoing open heart surgery.
Acknowledgments
The authors would like to thank Miss Julia Edwards for her assistance in the statistical analysis.
References
Footnotes
MC and KP contributed equally.
Contributors MC: chief investigator, responsible for study conception; surgical expertise and responsible for delivering the intervention to participants. Overall responsibility for the study. Corresponding author KP: responsible for preparing the statistical analysis plan, with advice from CAR, undertaking analyses and preparing a first draft of the manuscript. SB: managed the trial, including protocol amendments and reports. KSh: responsible for approaching and recruiting patients. KSe: responsible for approaching and recruiting patients. LE: managed the trial, including site initiation. SS: co-investigator with surgical expertise and responsibility for delivering the intervention to participants. AP: co-investigator with surgical expertise and responsibility for delivering the intervention to participants. GC: carrying out analyses and producing tables and graphs. LC: provided trial management expertise and advice. GDA: co-investigator providing surgical expertise. RP: co-investigator with surgical expertise and responsibility for delivering the intervention to participants. CAR: co-investigator with responsibility for delivering the study results and report; critical review of the drafted manuscript.
Funding The British Heart Foundation, Cardiovascular theme of NIHR Bristol Biomedical Research Centre and Garfield Weston Trust, supported this work. This study was designed and delivered in collaboration with the Clinical Trials and Evaluation Unit, a UKCRC registered clinical trials unit which, as part of the Bristol Trials Centre, is in receipt of National Institute for Health Research CTU support funding.
Competing interests None declared.
Patient consent Parental/guardian consent obtained.
Ethics approval Thermic-1: North Somerset and South Bristol, reference E4766; Thermic-2: South West—Central Bristol, reference 11/SW/0122.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There is no additional data; everything is included in the supplement.