Article Text

Statistics from Altmetric.com
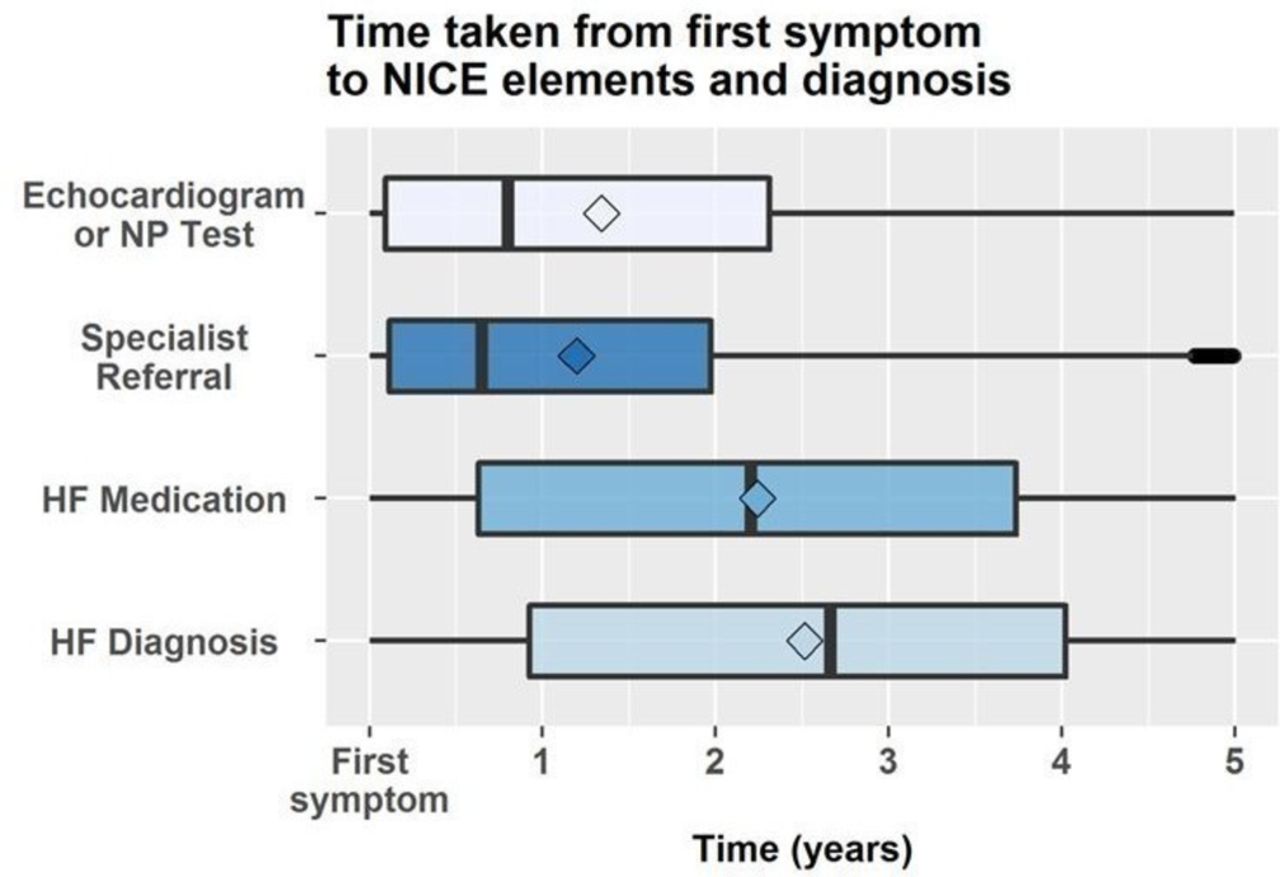
Most patients with new-onset heart failure (HF) will present to a primary care provider with symptoms of fatigue, breathlessness and ankle swelling. Diagnosis can be challenging given the nonspecific nature and frequency of these symptoms in the general population as well as time constraints and competing primary care issues. In an effort to understand current adherence to recommended pathways for diagnosis of HF in primary care, Hayhoe and colleagues1 linked primary and secondary care data from the UK Clinical Practice Datalink. Of the over 42 thousand patients diagnosed with HF over a 4 year time period, about 40% presented to a primary care provider with HF symptoms. However, only 39% underwent echocardiography or a serum natriuretic peptide test, with an average delay of almost 10 months from symptom onset to diagnostic testing and a total delay from symptoms to HF treatment over 2 years. (figure 1) Factors resulting in longer time delays included female sex, older age, higher deprivation scores, and fewer comorbidities.
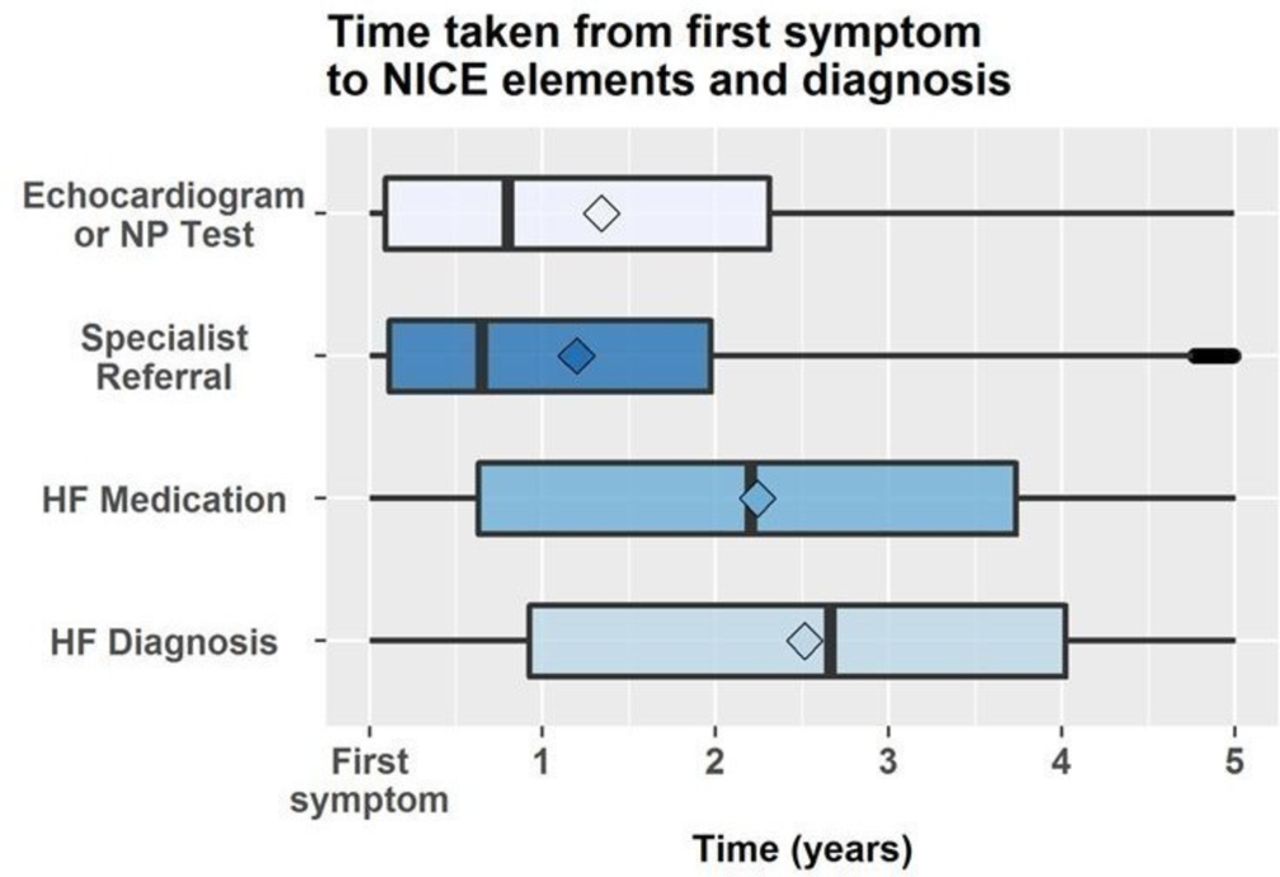
Timings from recorded symptom to investigation, referral and diagnosis. HF, heart failure; NICE, National Institute for Health and Care Excellence; NP, natriuretic peptide.
Taylor2 puts these findings in context by pointing out that 3%–4% of the National Health Service budget in the UK goes towards HF diagnosis and treatment. As she so clearly states: ‘Large clinical trials have established the clinical and cost-effectiveness of disease-modifying drugs and device therapies in improving quality of life, reducing hospitalisations and increasing survival for patients with HF with reduced ejection fraction.’ ‘Primary care has a vital role in HF diagnosis to allow timely initiation of evidence-based treatments which improve both patient outcomes and resource use in the healthcare system. More work is required to understand general practitioner consultations with people presenting with HF symptoms and identify organisational barriers such as access to investigations and secondary care waiting times which may contribute to delay.’
Another interesting paper in this issue of Heart is a meta-analysis of cohort studies examining the association between inflammation and hypertension. Based on data from 21 studies with over 142 thousand patients, Jayedi and colleagues3 found that elevated circulating inflammatory markers were associated with an increased risk of future hypertension. For example, the risk ratio from the third versus first tertile of C-reactive protein was 1.23 (95% CI 1.11 to 1.35) with the analysis showing a linear increase in risk of hypertension with increasing inflammation marker levels, across the entire data range (figure 2).

Dose-response associations between circulating inflammation markers and risk of developing hypertension. CRP, C reactive protein; hs-CRP, high-sensitive C reactive protein.
In an editorial, Knutsor and Laukkanen4 point out the additional association between cardiorespiratory fitness (CRF), inflammation and hypertension with previous studies suggesting ‘that high CRF may attenuate the association between CRP and incident hypertension, especially among those with initially elevated CRP levels.’ They conclude: “While we await more convincing evidence on the potential relevance of inflammatory pathways in hypertension prevention, lifestyle measures such as engaging in regular physical activity; maintaining a good CRF level and healthy body weight; salt restriction; limitation of alcohol consumption; high consumption of vegetables and fruits; a low-fat diet; and elimination of smoking should remain the cornerstone for the primary prevention of hypertension.’
Two other research papers in this issue focus on women with Turner syndrome (TS). In a single centre study of 268 TS patients, computed tomographic or MRI showed aortic dilation was present in 22% and associated with hypertension, a bicuspid aortic valve (BAV), 45XO karyotype and growth hormone treatment.5 Only 2% of patients suffered aortic dissection or required aortic surgery over the 7 year follow-up period. In a separate study, coronary artery anatomy was left dominant in about 25% of 86 TS patients, both in those with a BAV or normal trileaflet valve.6 However, BAV patients with fusion of the right and left coronary leaflets more often had left coronary artery dominance both in TS patients and controls with an isolated BAV. About 10% of TS-BAV patients had an absent left main coronary artery (figure 3).

{kind=link}
{kind=link}
{kind=link}
Example of bicuspid aortic valve with fusion of right and left coronary leaflets (RL BAV) without raphe, closed (A) and open (B), with separate ostia (arrows) of the left anterior descending coronary artery (LAD) and left circumflex artery (LCX) (C). (D, E) Three-dimensional reconstruction of a heart with RL BAV without raphe, aortic coarctation (CoA), a left dominant coronary artery system and separate ostia of the LAD and LCX. The aortic valve is indicated in yellow. Ao, aorta; LA, left atrium; LV, left ventricle; PDA, posterior descending artery; PT, pulmonary trunk; RA, right atrium; RCA, right coronary artery; RV, right ventricle; RVOT, right ventricular outflow tract.
The Education in Heart article in this issue7 discusses the role of simulation-based education in cardiology. Barakat emphasises that ‘Simulation-based education is a technique not a technology’ and that “the benefits in simulation-based education in reducing patient risk through human factors training is probably greater than its potential benefits in manual skills acquisition.’ Simulation-based approaches certainly have the potential to allow more rapid achievement and documentation of competency in all aspects of medical care.
The Image Challenge question shows an unusual and interesting finding in a patient undergoing a cryoablation procedure for atrial fibrillation.8 Be sure to look at the online video!
Footnotes
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.
Patient consent for publication Not required.