Article Text

Abstract
Coronary events remain a major cause of sudden incapacitation, including death, in both the general population and among aviation personnel, and are an ongoing threat to flight safety and operations. The presentation is often unheralded, especially in younger adults, and is often due to rupture of a previously non-obstructive coronary atheromatous plaque. The challenge for aeromedical practitioners is to identify individuals at increased risk for such events. This paper presents the NATO Cardiology Working Group (HFM 251) consensus approach for screening and investigation of aircrew for asymptomatic coronary disease.
A three-phased approach to coronary artery disease (CAD) risk assessment is recommended, beginning with initial risk-stratification using a population-appropriate risk calculator and resting ECG. For aircrew identified as being at increased risk, enhanced screening is recommended by means of Coronary Artery Calcium Score alone or combined with a CT coronary angiography investigation. Additional screening may include exercise testing, and vascular ultrasound imaging. Aircrew identified as being at high risk based on enhanced screening require secondary investigations, which may include functional ischaemia, and potentially invasive coronary angiography. Functional stress testing as a stand-alone investigation for significant CAD is not recommended in aircrew. Aircrew identified with coronary disease require further clinical and aeromedical evaluation before being reconsidered for flying status.
- cardiac imaging and diagnostics
- cardiac risk factors and prevention
- health care delivery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Despite advances in prevention and early disease intervention, ischaemic coronary events secondary to coronary artery disease (CAD) remain among the most common causes of acute incapacitation in the Western world. Although aircrew are medically monitored more intensively than many other professions and cockpit resource management with incapacitation training have reduced the rate of major aircraft accidents, acute coronary syndromes (ACS) are still causative of the most common causes of commercial pilot incapacitation resulting in aircraft accidents and fatalities.1 2 Table 1 lists some examples of accidents and incidents in commercial passenger flights over the past 40 years related to cardiovascular events. Despite the presence of multiple pilot crews, cardiac events still have a significant impact on flight operations. i ,ii
Examples of aircraft accidents and incidents related to coronary events
Military air operations, in contrast to commercial flights, are often conducted in single-pilot, high-performance aircraft, and even in dual-pilot military operations full attention of both pilots is required in many phases of the mission, with potentially catastrophic outcomes resulting from incapacitation of either. In the US Air Force (USAF), cardiac events have historically been the second most common cause, after neurological events, of aircraft accidents secondary to acute incapacitation.3 4
Coronary atherosclerosis is a systemic and progressive disease that begins in young adults. The vast majority of ACS and sudden cardiac deaths (SCDs) in this younger population occur unheralded. In recent years, the aetiology of ACS in younger people has been clarified, although incompletely. Few, if any, aircrew involved in accidents and incidents suffer from antecedent symptomatic coronary disease. However, we know that CAD is prevalent in aircrew. Autopsy studies of young military personnel and aircrew have demonstrated atherosclerosis as a common finding, including cases of severe disease and aeromedically disqualifying findings.5–8 In contrast to progressive atherosclerotic disease gradually leading to luminal occlusion with antecedent symptoms, as is seen in traditional cases of ischaemic heart disease (IHD), most coronary events that occur in younger individuals occur because of the rupture of non-flow-limiting coronary plaques, or superficial erosion of remodelled plaque.9 10 This triggers an intravascular coagulation cascade leading to acute thrombus formation that obstructs the coronary lumen. Although fewer in number, accidents also occur in aircrew returned to flying following a coronary intervention; even in these individuals who have had interventions such as percutaneous coronary intervention or coronary artery bypass grafts, ACS often occurs due to plaque rupture at a different site, remote from the revascularised artery.
The further understanding of the aetiology of ACS has changed the way we define coronary disease, and concurrently, the preferred approach for screening and investigation. Since most ACS events arise from rupture or erosion of non-obstructive coronary plaque, dynamic screening tests aimed at detecting obstructive coronary disease have significant limitations when used as screening tools for vulnerable atherosclerotic plaque in this aircrew cohort.
Due to our advancing knowledge, recent attention has increasingly focused on the nature of the atherosclerotic plaque. Histopathology studies of plaques prone to rupture have shown that the thickness of the fibrous cap is the best discriminator of likelihood of rupture.11 While no current clinical imaging techniques can accurately identify cap thickness and plaque composition, recent advances in CT coronary angiography (CTCA) and cardiac MRI (CMR) show promise in the identification of high-risk plaques.12
Many coronary events occur in individuals with normal lipid levels, and with no clear evidence of intravascular inflammation. Genetics and hereditability also appear to play an important role suggesting as-yet-undiscovered aetiological metabolic pathways.
The purpose of this paper is to outline a broad consensus approach to screening for coronary disease in asymptomatic aircrew and to provide recommendations for further investigating aircrew identified as being at increased risk for a coronary event.
Approach to screening for asymptomatic CAD
So how can aeromedical physicians identify individuals with vulnerable plaque who are at increased risk for an ACS event? The issue of how best to screen for aviation-relevant CAD has been an aeromedical challenge for decades, with screening recommendations evolving as newer, more refined and evidence-based tools become available. Generic tools for screening and investigation should ideally be inexpensive, readily available locally, reliable, and ideally provide good discrimination between those at risk and those not.
Unfortunately, for most screening tools, including basic risk assessment calculators and enhanced screening tools such as exercise ECGs, there is considerable overlap in positive and negative test results between the two populations, with resulting difficulty in discriminating between those with and those without disease. Screening tests with lower specificity (and therefore lower negative predictive value) are likely to produce higher rates of false positives when applied to a population with relatively low disease prevalence (such as significant CAD in aircrew). For functional tests such as exercise ECG with a specificity of 60%–70% at best, it is more likely that a positive stress ECG will be false positive than to reflect an obstructive coronary lesion. This potentially leads to further unnecessary investigations that may be associated with risks such as a radiation exposure, procedural risks from intervention or additional incidental findings that require extensive further investigation. In aircrew, this may result in removal from flight duty and delays in appropriate disposition with related impact on operational effectiveness and subsequent cost ramifications.
One of the challenges of assessing CAD risk in aircrew is determining which test to apply and when, which tests should be routine, and when should enhanced screening tests (to further define the risk) or investigation (to visualise directly the coronary anatomy or assess the physiological effects of any potential coronary obstruction) be performed.
Initial screening
Initial screening tools to assess cardiovascular risk include standardised risk estimation calculators and the standard 12-lead ECG. Risk estimate calculators provide a good first approach to assessing cardiovascular risk in those without a previous cardiovascular history, providing risk-stratification, identifying those most likely to benefit from primary prevention, and, for aeromedical purposes, identifying those at potential excess risk for an ACS in whom further enhanced screening or investigation may be appropriate. Although the routine 12-lead ECG is not a good discriminator of significant CAD in isolation, it may reveal abnormal conduction patterns such as left bundle branch block that may raise the possibility of occult CAD, or reveal inherited diseases such as long QT and Brugada syndromes, hypertrophic cardiomyopathy, right ventricular cardiomyopathy, and other conditions that could increase the risk of sudden death in aircrew.
Various risk equations are available and easily accessible on-line. They include, to name but a few, the Framingham Risk Score, PROspective CArdiovascular Münster study (PROCAM), ArbeitsGruppe Lipide und Atherosklerose (AGLA), QRISK, Reynold’s Risk Score (RRS) and SCORE.13 Most have been constructed with data from populations in North America and Europe, are generally population-specific, and may not be well calibrated for other populations.14 15 Additional limitations of risk calculators for the risk assessment of many aircrew" after calculators include higher subject age range (such as Framingham Risk Score that has a minimum age of 45 years) and the use of hard end points (such as, myocardial infarction and SCD) which may limit applicability in aircrew, where ACS and other causes of potential incapacitation or distraction are important. Risk calculators usually provide estimations of risk over 5–10 years or longer and are provided as per cent risk per decade for events. The interpretation of these statistics requires both an understanding as to what exactly the percentage risk is for an individual, and caution when considering risk in an individual aircrew from population-based data. The calculated result does not mean that any particular individual has the defined percentage risk/decade for an event, but rather that for 100 individuals with similar characteristics that defined percentage will have an event.
The ability of risk estimate equations to identify those at increased risk for cardiovascular events (calibration) varies considerably and calculators often overestimate likelihood of event rate. DeFilippis16 found that of five commonly used risk calculators in the USA, four (FRS-CHD; FRS-CVD; Adult Treatment Panel III-Framingham Risk Score-Coronary Heart Disease (ATPIII-FRS-CHD); American Heart Association-American College of Cardiology-Atherosclerotic cardiovascular disease (AHA-ACC-ASCVD)) overestimated the risk for cardiovascular end points, compared with true outcome data from the large The Multi-Ethnic Study of Atherosclerosis Trial, by 53%, 37%, 154% and 86%, in men, respectively. The overall discordance between observed and predicted cardiovascular events was lowest at −3% for RRS, a calculator that includes family history and high-sensitivity C reactive protein (hs-CRP) as variables.
Despite their limitations, the application of a risk calculator best calibrated to the particular population relevant to an individual aircrew remains the best initial approach to identify aircrew at increased cardiovascular risk. Risk-stratification using risk equations increases the pretest probability for any subsequent investigations, and as per Bayes’ theorem, increases the post-test probability of a true positive result. The decision as to which risk calculator is most appropriate should be based on specific factors of the population being screened, but should include consideration for age, ethnicity and gender. Onset of angina/ACS symptoms is a significant aeromedical event, and ideally, the risk calculator should include both non-fatal and fatal end points. Family history and hs-CRP both appear to be significant markers of risk, and should be included in the overall estimated risk, if not included in the risk equation used. This is an evolving field and newer risk calculators are being developed all the time. For example, The Astronaut Cardiovascular Health and Risk Modification (Astro-CHARM) is a new risk equation based on pooled cohort data in individuals aged 40–65 years which may be more appropriate for aircrew populations17 18 and has been used by NASA in assessing risk in its astronaut population.
Initial screening for coronary artery disease in aircrew
Enhanced screening
Aircrew identified as being at increased cardiovascular risk based on initial screening should undergo enhanced screening. Enhanced screening may include additional testing with stress ECG, coronary artery calcium scoring alone, or combined with a CTCA investigation, and vascular ultrasound imaging (VUI).
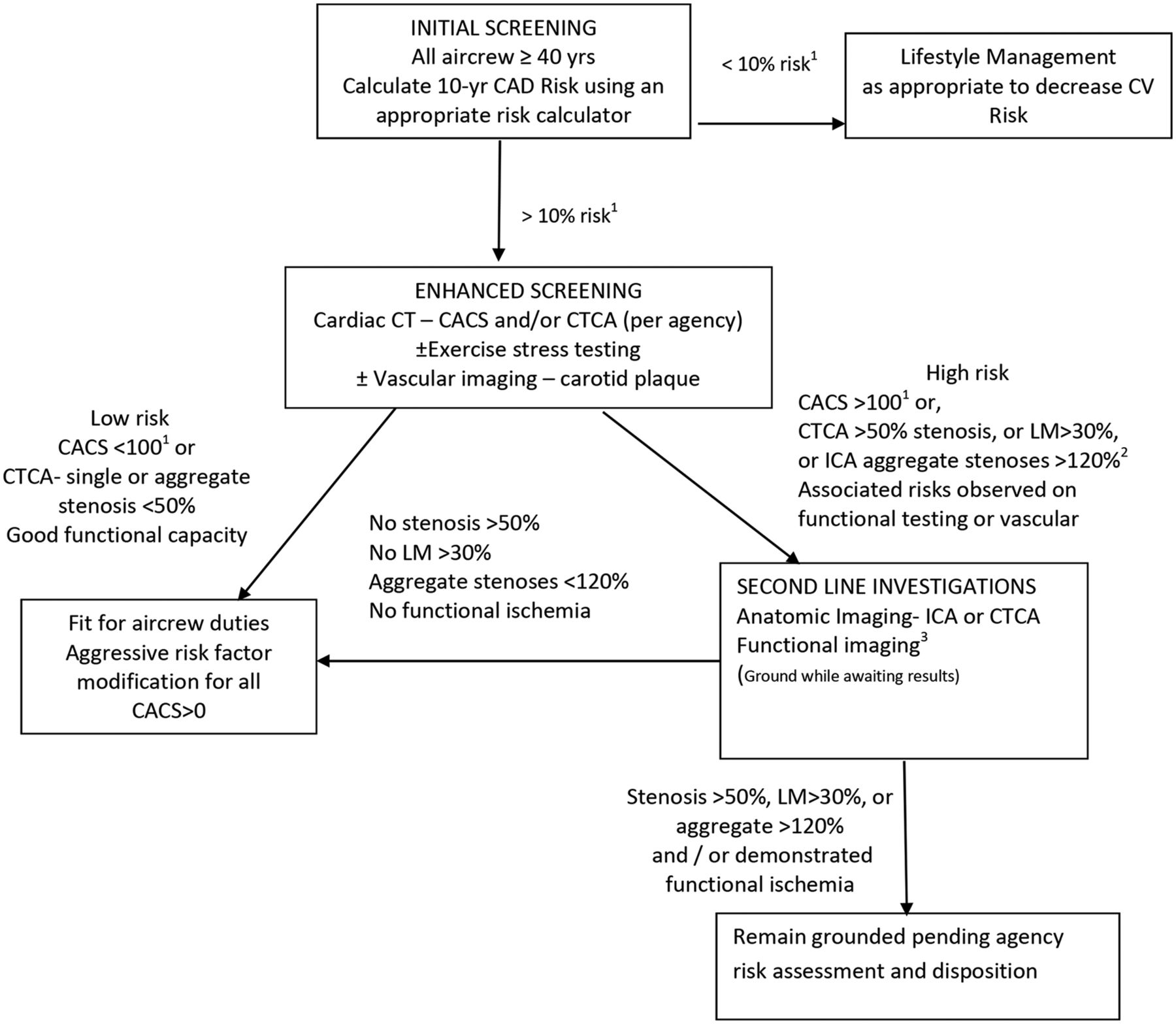
The threshold for initiating enhanced screening of aircrew with increased estimated risk for a coronary event is an organisational decision. Lower thresholds will result in higher rates of additional testing, with more false-positive results while higher thresholds risk missing aircrew with disease. Ideally, thresholds should be context-specific and based on specific risk assessment models. A 10%/decade threshold to initiate enhanced screening is recommended (see figure 1), but the particular threshold and risk acceptance, should be determined by the regulatory agency.

{kind=link}
HFM-251 generic screening and evaluation algorithm (Adapted from DeJohn et al [1]). (1) This algorithm should be modified/revised for use by specific agencies as required. (2) Aggregate stenosis is the sum of quantified stenoses found on invasive coronary angiography (ICA). Adapted from Davenport et al [53]) (3) Functional imaging refers to stress myocardial function (eg, MUGA), stress nuclear perfusion studies stress echocardiography or perfusion CMR. Functional imaging should be performed based on the results of anatomical imaging studies and/or clinical decision. CAD, coronary artery disease; CACS, Coronary Artery Calcium Score; CTCA, CT coronary angiography; MUGA, multigated acquisition.
Coronary Artery Calcium Score
Exercise stress tests are limited in their ability to detect potentially flow-limiting CAD19 and to predict future cardiovascular events. Historic USAF data, beginning in the 1970s, demonstrated that over a period of 20 years, treadmill testing, with or without myocardial perfusion scintigraphy (MPS) using thallium, was a poor predictor of cardiovascular events in USAF aircrew (table 3).20–22 The presence or absence of coronary artery calcium as demonstrated by fluoroscopy performed much better at predicting angiographic coronary disease23 and events.
Annualised cardiac event rate over 5 years (revascularisation, MI, cardiac death) in US Air Force (USAF) aircrew based on treadmill, thallium and fluoroscopy test results
Furthermore, USAF aviators with a positive treadmill, thallium MPS or fluoroscopy were required to undergo coronary angiography in order to be cleared to return to flying duties. Of 1487 aviators who underwent catheterisations, 929 were assessed as normal (no detectable lesions), 249 had mild disease (<50% lesions), 124 had moderate disease (50%–70% lesions) and 185 had severe disease (>70% lesions). Coronary calcium detected by fluoroscopy showed a higher sensitivity, specificity and positive predictive value for detecting severe (>70%) lesions demonstrated on invasive coronary angiography (ICA). However, all three modalities investigated had a relatively poor positive predictive value (table 4).
Results of investigations in detecting significant angiographic lesions (>70%) in US Air Force (USAF) aircrew
In the late 1980s, fluoroscopic imaging of coronary arteries for calcium segued to CT scanning for Coronary Artery Calcium Scores (CACS)24 25 allowing a more formal, reproducible quantification of calcified plaque, as the Agatston Score, or alternatively, a Volumetric Score. Over the past 20 years, increased CACS have correlated with increased cardiovascular events and CACS may result in reclassification of risk based on traditional calculations.26
CACS better quantifies risk as it reflects overall coronary plaque burden;27 calcium is thought to represent approximately a fifth of the total atheroma burden28 so the more calcified plaque, the more likely an individual is to have separate, non-calcified plaque that is more vulnerable to rupture.29 Calcium deposition occurs as plaque matures and stabilises, and it is unlikely that it will be the calcified plaque that ruptures. With aggressive risk factor modification, such as statin therapy, calcium scores may paradoxically increase, while the risk of plaque rupture decreases. In those not on secondary prevention, an increasing Agatston Score correlates with increased plaque burden, coronary stenosis and coronary event rates, as shown in table 5.30
Event rates for revascularisation, myocardial infarction and sudden cardiac death (SCD) with various coronary calcium scores in over 32 months in 1153 patients, median age 58 (±10) years30
One caveat to low coronary calcium scores for risk-stratification is that while on a population basis, a calcium score of 0 is clearly associated with a very low risk for a coronary event, the risk is not zero. Not all plaque is calcified, and plaque rupture events may occur in individuals with only non-calcified plaque. In a recent review of 44 Royal Air Force aircrew who underwent both CACS and CTCA (most commonly after a positive exercise stress test), two patients who had CACS <10 had at least one stenosis ≥50% on CTCA, including one patient with a CACS of 0 and a critical LAD stenosis on both CT and ICA.31 At a population level, event rates for coronary calcium scores of 0 are very low, with mortality <0.1%/year,32 but although the event rate is very low, the absence of coronary calcium does not necessarily exclude aeromedically significant atherosclerotic plaque.
Therefore, for aircrew identified as other than low risk based on traditional risk factor estimation, CACS provides a better estimation of future risk for a cardiac event than functional testing, and is the preferred modality for enhanced screening alone or combined with a CTCA investigation. For space flight participants travelling to the International Space Station (and International Space Station (ISS) crew members), CACS is a required primary screening test.33 A generic screening algorithm, which may be modified for use by aeromedical agencies, is provided in figure 1.
CT coronary angiography
Historically the only accurate way to visualise the coronary artery lumen was with ICA. Fortunately, with advances in cardiovascular CT technology, CTCA has evolved into a clinically recommended alternative. Unlike CACS, CTCA provides information about the number, extent and location of luminal stenoses. It additionally has the advantage of being able to both image and characterise plaque (into calcified, non-calcified or mixed plaque morphology). This allows identification of plaque disease that may be present in significant quantities even with very low/no coronary calcium demonstrated on a CACS scan. CTCA may thus identify individuals with low coronary calcium scores who are nevertheless at increased risk for coronary events.31 34 35 Additionally, CTCA is able to visualise early plaque deposition which is subendothelial and expands outwards through GLAGOV (positive) remodelling, with little or no encroachment on the lumen. Only after maximal outward expansion does luminal encroachment occur. Positive remodelling, non-calcified plaque burden and other high-risk plaque morphologies are all associated with a higher likelihood of ACS, even in those with minimal and moderate luminal stenoses.36 Importantly, functional testing in such individuals will usually be negative.
The process of obtaining a CTCA is more complex than a simple CACS; it requires an intravenous contrast injection, and often IV β-blocker administration to slow the heart rate to optimise image acquisition. In patients with high calcium burden, CTCA may overestimate luminal encroachment (especially with a CACS of >1000). For CTCA, the presence of obstructive lesions greater than 50% is a reasonable aeromedical threshold for grounding and further investigation.
Novel techniques allow derivation of accurate CACS from CTCA studies, thus providing more information while minimising radiation exposure.37 For some aircrew identified as being at high risk based on enhanced screening, a cardiac CT protocol that provides both CTCA and CACS information may be the preferred modality.
Cardiovascular CT is associated with a small incremental risk related to radiation exposure that is potentially higher than with a CACS (although with modern scanners and with low dose acquisition protocols, this may not always be the case). With modern scanners, the dose from a CTCA is between 2 mSv and 4 mSv38 and from CACS between 0.5 mSv and 1 mSv.39 To put these doses in context, and for comparison, commercial airline cabin crew would expect to receive 2–3 mSv radiation per annum from cosmic rays, and the background radiation dose in the UK ranges between 2 mSv and 7 mSv.40 Other commonly used cardiovascular imaging tests described in this manuscript also involve ionising radiation with typical doses between 3 mSv and 5 mSv for ICA and 5 mSv and 15 mSv for nuclear perfusion or function studies.
Exercise stress testing
Although exercise stress ECG has shortcomings as a screening tool for coronary atherosclerosis because of its limited sensitivity and specificity, it does provide useful risk-stratification information, blood pressure response to exercise, observation of exercise-related arrhythmias, and importantly, measurement of aerobic fitness. Coronary event risk is inversely proportional to aerobic fitness,41 and a good level of aerobic fitness significantly reduces predicted coronary event rates. While in a low-prevalence population, exercise stress ECG suffers from a low positive predictive value for the determination of coronary events, a normal maximum-effort exercise treadmill test demonstrating a good level of aerobic fitness has significant negative predictive value for aeromedical disposition considerations. Because stress tests are readily available, are relatively inexpensive and provide useful information beyond testing for exertional ischaemia, many agencies use stress testing as a first-line test in individuals deemed to be at increased risk of cardiovascular disease. However, due to the limited sensitivity of the exercise ECG (60%–70%),19 of 100 individuals with angiographically demonstrated obstructive coronary disease, the exercise stress ECG will be normal (negative) in 30–40 cases. Additionally, the exercise ECG has a very low positive predictive value for future coronary events. For this reason, stress ECG should be discouraged as a stand-alone tool to determine aeromedically significant CAD.
Vascular ultrasound imaging
Ultrasound imaging of the carotid and femoral arteries provides easily accessible visualisation of vascular anatomy without radiation. Carotid intima-media thickness (IMT) and carotid and femoral artery plaque, have been evaluated as markers for cardiac disease and stroke risk. Several prospective studies have shown that the presence of carotid and femoral bifurcation plaques is associated with future cardiovascular events, independent of other risk factors. While IMT is associated with an increased risk for stroke, a recent meta-analysis of these and other studies demonstrated the superiority of measuring plaque over IMT in cardiac risk prediction.42 The American Heart Association/American College of Cardiology43 and the European Society of Cardiology44 guidelines support the use of carotid artery ultrasound in the cardiovascular risk assessment of asymptomatic adults at intermediate risk.
From an aeromedical perspective, VUI can be used in several ways. First, together with traditional risk factors, it may be incorporated into an enhanced screening programme to identify aircrew at increased risk, providing incremental independent risk information. Second, in assessing aircrew identified as being at intermediate risk based on traditional risk factors, carotid and femoral vascular imaging for plaque can provide helpful information that may allow reclassification to high risk or low risk as an intermediate step before pursuing radiation-based imaging studies. Thirdly, VUI can be used in a serial fashion to monitor the effects of interventions on atherosclerotic plaque.45
Second-line investigations for CAD assessment
In aircrew whose enhanced screening investigations suggest the presence of significant CAD, further investigation is warranted to maintain flying status. Further investigations generally involve functional assessment for inducible ischaemia and may require direct anatomical imaging with angiography to better define the risk of an acute coronary event.
Functional imaging
Functional assessments for inducible ischaemia may include myocardial function studies (global ejection fraction, regional wall motion abnormalities) and myocardial perfusion analysis, with either stress echocardiography, CMR or nuclear imaging. Due to the lack of radiation exposure, stress echocardiography and perfusion CMR may be preferred to nuclear MPS in younger subjects. All functional modalities have significant data (although not in aircrew populations) to support their use. A negative MPS gives a ‘warranty’ period, where the likelihood of a significant cardiovascular event is thought to be <1% per annum, for 3 years.46 However (as previously discussed), functional imaging, in isolation, has been shown to be of limited value in predicting aeromedically significant CAD.
The role of ICA
ICA currently remains the gold standard for anatomical imaging of coronary arteries. This is because the spatial resolution of ICA is superior to that of CTCA. CTCA is less accurate than ICA for quantifying luminal stenosis. To put this in context, a 50% stenosis found on CTCA may be in the region of 30%–70% at autopsy, while a 50% stenosis on ICA will be between 40% and 60%.38 Caution should therefore be applied in the interpretation and comparison of ICA and CTCA data when rigid cut-offs are recommended for determination of suitability to fly. The use of ICA is however problematic in aircrew for a number of reasons; first, ICA is associated with a risk of stroke, MI, coronary dissection and vascular access damage in as many as 1 in 30 cases.47 48 The overall risk of death with ICA is approximately 1 in 1000. Second, ICA is more expensive and often not immediately available. Because of these concerns, ICA is preferably undertaken on clinical indications for individuals likely to require intervention. Its use in an occupational context requires appropriate discussion and consent from the patient concerning risks and benefits, given the possible career implications of a procedure-associated event.
Emerging technologies
CMR for plaque imaging
CMR has been used for over a decade to image carotid plaque as a risk factor for stroke,49 but CMR of coronary plaque has been constrained by the size and movement of coronary arteries. Although CMR is inferior to CT for imaging coronary vascular anatomy, there is increasing interest in the application of MRI techniques for identifying vulnerable coronary plaque. For example, Noguchi et al 50 showed that high-intensity plaque identified by non-contrast T1-weighted imaging with increased plaque-to-myocardium signal intensity ratio was an independent predictor of coronary events. While CMR is, at present, not suited to assessment of aircrew with risk factors, MRI techniques including Positron emission tomography (PET)/MRI and stress perfusion MRI may, in the future, play a role in the evaluation of aircrew with known coronary disease in an overall risk assessment for future cardiac events in consideration for a return to flying duties.
Fractional flow reserve
Fractional flow reserve (FFR) is a technique traditionally used as an adjunct to ICA to measure pressure differences across coronary stenosis. This determines the likelihood that the stenosis is functionally significant. FFR is defined as the pressure distal to a stenosis relative to the pressure before it. This results in absolute quantification; an FFR of 0.80 defines a stenosis causing a 20% drop in pressure across the lesion. This is the cut-off used to determine clinical significance. FFR has been shown to be more accurate than visual assessment of functional lesions on ICA.51 FFR expresses the maximal flow down a vessel in the presence of stenosis compared with the maximal flow in the hypothetical absence of stenosis. More recently FFR has been developed for use with CTCA data sets. FFRCT is based on complex computational flow dynamics and may allow assessment of physiologically significant stenoses identified on CTCA.52 While FFR on ICA is used to determine the requirement for intervention clinically, it is the role of FFRCT that is of most interest in aviation medicine as it may help overcome some of the limitations of overestimation of severity of stenosis on CTCA. Currently, however, the technology requires very significant computing power and remains a promising research application.
Aeromedical disposition
Aircrew identified as being at high risk for a coronary event based on the presence of extensive coronary atherosclerosis on imaging should be removed from aircrew duties and are required to undergo further cardiological evaluation before returning to flying duties. The CACS threshold for requiring angiography (CTCA or ICA) is an organisational decision, related to the defined threshold for acceptable risk. However, a coronary calcium score of 100, at a population level, is an established clinical threshold above which the probability of obstructive disease and coronary events becomes moderately elevated, with event rates exceeding 1%/yr.
Aircrew at lower risk for a coronary event do not necessarily require an operational restriction, but do require intensive risk factor modification that includes all modifiable risk factors, including smoking cessation, blood pressure control, encouragement to increase aerobic fitness and consideration for statin medication. If used in isolation, a CACS greater than 100 should result in aircrew being temporarily removed from operational duties pending further investigation. If the CACS is greater than 400, consideration should be given to invasive angiography as CTCA may be non-diagnostic, and if CACS is greater than 1000, CTCA is not recommended.
Returning individuals with known coronary disease to flight duties requires detailed risk evaluation including control of modifiable risk factors. Other papers in this series address these issues in more detail.
Discussion
Major adverse coronary events among aircrew continue to be a threat to aviation safety and military air operations. Understanding of the process of atherosclerosis has evolved with clarification that the rupture of a thinly capped, generally non-obstructive plaque is often the aetiology of ACS, particularly in younger people. This has shifted the paradigm for screening aircrew for coronary disease. Functional tests, meant to detect myocardial ischaemia because of obstructive lesions, do not detect atherosclerotic plaque until advanced, obstructive disease occurs and have limited utility in an aeromedical cardiovascular screening programme. Exercise stress testing is equally limited in this sense but provides useful ancillary risk-stratification information including blood pressure response to exercise and an objective measure of aerobic fitness. Other modalities such as CACS and VUI can provide additional helpful information in an enhanced cardiovascular screening programme.
For aircrew identified as being at increased cardiovascular risk based on a risk estimation and/or an enhanced screening programme, CT imaging provides a better assessment of cardiovascular event risk than functional testing. Both CT CACS and CTCA provide validated, evidence-based risk-stratification information. CACS has some advantages over CTCA in that it is inexpensive, is reproducible and does not require intravenous contrast. Acquisition and scoring protocols are standardised, however CACS data are population-based and provide no detail on extent and location of luminal narrowing in an individual subject. CTCA potentially allows determination of individual risk; however, it may be less accessible and where extensive calcification exists there is increased interobserver variability. Both techniques have an extensive evidence base relating to future coronary risk.
Importantly, the absence of calcified plaque does not guarantee the absence of significant, even obstructive coronary atheroma and coronary events do occur in individuals with zero or very low CACS. CTCA technology is evolving and now permits the calculation of CACS from within a CTCA data set. The choice of which imaging modality to use (CACS or CTCA) is primarily an organisational decision. Both modalities provide useful, quantitative information.
Summary
Identifying potentially significant coronary artery disease in aircrew is of paramount importance in maintaining flight safety and protecting aircrew form symptoms that may lead to flight critical distraction and/or incapacitation. The classes of recommendation are derived from the European Society of Cardiology definitions. A suggested flow chart is shown at figure 1; the exact cut-off for additional investigation will be an individual agency decision based on their specific acceptable levels of risk.
Enhanced screening for coronary artery disease in aircrew
Exercise stress testing in aircrew
Vascular ultrasound
Functional imaging in aircrew assessment
Invasive Coronary Angiography
Supplementary file 1
References
Footnotes
↵ i Preamble: Evidence-based cardiovascular risk assessment in aircrew poses significant challenges in the aviation environment as data to support decision making at the low level of tolerable risk in aviation is rarely available from the published literature. As a result, there are discrepancies between the aviation authority’s recommendations in different countries, and even between licensing organisations within single countries. The NATO HFM-251 Occupational Cardiology in Military Aircrew working group is constituted of full-time aviation medicine and aviation cardiology experts who advise both their militaries and civil aviation organisations including, but not limited to, the Federal Aviation Administration (FAA), Civil Aviation Authority (CAA), European Aviation Safety Agency (EASA) and NASA. The recommendations of this group are a result of a 3-year working group that considered best clinical cardiovascular practice guidelines within the context of aviation medicine and risk principles. This work was conducted independently of existing national and transnational regulators, both military and civilian, but considered all available policies, in an attempt to determine best evidence-based practice in this field. The recommendations presented in this document, and associated manuscripts, are based on expert consensus opinion of the NATO group. This body of work has been produced to develop the evidence base for military aviation cardiology and to continue to update the relevant civilian aviation cardiology advice following the 1998 European Cardiology Society aviation cardiology meeting.
↵ ii Aircrew: Aircrew are defined somewhat differently in civil and military aviation. North Atlantic Treaty Organization (NATO) and International Civil Aviation Organization (ICAO) delegates the definition of aircrew to national authorities. In the civilian sector aircrew are often categorised as flight crew (pilots)/technical crew members and cabin crew, with separate regulation for air traffic controllers. The military define aircrew more broadly as ’persons having duties concerned with the flying or operation of the air system, or with passengers or cargo when in flight'. From a risk perspective, professional (commercial) pilots have a higher attributable risk than private pilots and non-pilot aircrew. Controllers are considered to have an attributable risk equivalent to professional pilots. From a cardiovascular perspective, aircrew whose flying role includes repetitive exposure to high acceleration forces (Gz) comprise a subgroup who, due to the unique physiological stressors of this flight environment, often require specific aeromedical recommendations. A more detailed description of aircrew is available in table 1 of the accompanying introductory paper on aviation cardiology (ref Intro paper).
Contributors All authors are part of the NATO Aviation Working Group and have contributed to the writing and revision of the manuscript.
Funding Produced with support from NATO CSO and HFM-251 Partner Nations.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Commissioned; externally peer reviewed.