Article Text

Abstract
Background As the population ages, more elderly patients are presenting with symptomatic coronary artery disease (CAD). However, there is lack of evidence regarding the best therapy in this population especially with increasing frailty.
Purpose To determine the relationship between frailty and quality of life (QoL) of octogenarian patients presenting with symptomatic CAD.
Methods We enrolled 150 consecutive unselected patients aged ≥ 80, presenting with acute coronary syndromes and stable angina (SA). Assessments were done at baseline for frailty using Fried frailty phenotype (FFP) and Edmonton frailty scale (EFS). QoL was assessed using Short survey form (SF-12). Comorbidity was quantified using Charlson’s comorbidity Index. After the participants had undergone their respective treatments they were reassessed for frailty and quality of life at 4 months.
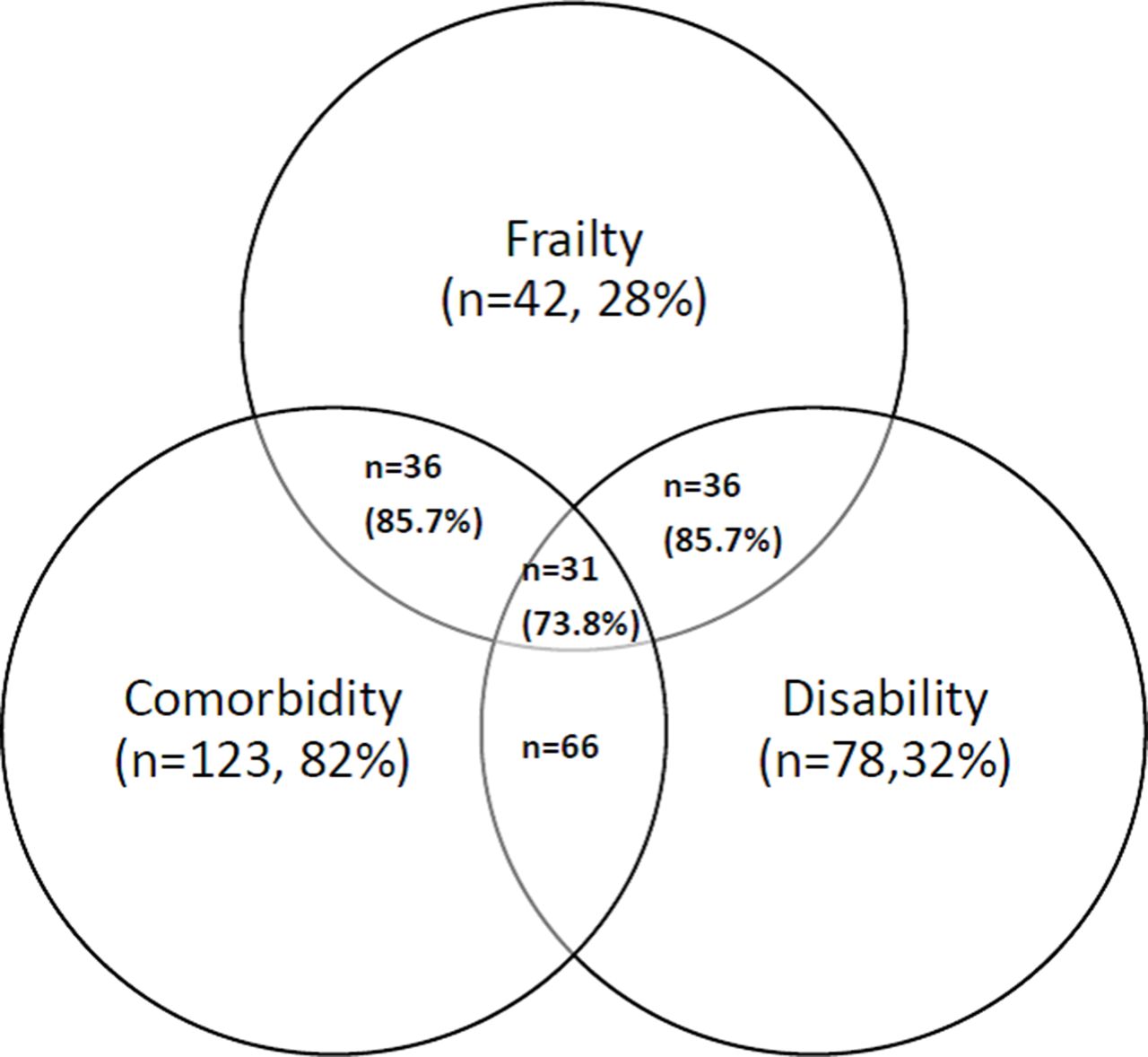
Results The mean age was 83.7±3.2 years. Ninety-nine (66%) of the participants were male. Average Charlson’s comorbidity index was 6.5±2.2. There was significant overlap between frailty comorbidity and frailty (73.8%) fig. 2. Presentation was Stable angina in 68(45.3%), NSTEMI 45(35%), STEMI 21(14%), and unstable angina 16(10.7%). Treatment was PCI in 51(34%), 15 (10%) underwent CABG surgery and 84 (56%) were treated medically. Frailty was present in 26% and 28% by EFS and FFP respectively and was more prevalent in females (FFP 37.3% vs 23.3% p=0.07, EFS 41.2% vs 18.2% p=0.03). Frail participants had higher symptom burden. Regression analysis showed that QoL was significantly related to frailty and Charlson’s comorbidity score. FFP was significantly related to the physical composite score for QoL, whilst EFS was significantly related to mental composite score for QoL (p=0.003). Frail patients with ACS had longer stay in hospital (6.5 vs 2.7 days, p=0.05). At 4 months, 14(9.35) had died, with frail participants having the lowest survival (50% vs 26.2% p=0.002). Of the remaining 136 participants, 103(75.5%) were re-assessed. There was a trend towards improvement in symptoms in all treatment arms but made no significant difference to frailty or QoL.

Kaplan-Meier Survival Curve (Fried Frailty Phenotype)
{kind=link}
{kind=link}
Abstract 158 Figure 2
Conclusion In octogenarians presenting with symptomatic CAD, frailty is significantly related to QoL and is a predictor of survival.
Conflict of Interest None