Article Text

Abstract
Introduction The combination of single antiplatelet and oral anticoagulation therapy demonstrated similar ischaemic efficacy when compared to triple therapy in patients with atrial fibrillation (AF) undergoing percutaneous coronary intervention (PCI).1,2 Importantly, a significant proportion of the included patients had bare-metal stents, up to one third, in these trials. 1,2 This may question the applicability of the reported data when tackling complex PCI in the real-world patients. We sought to investigate the incidence of ischaemic events in patients with AF undergoing PCI according to the complexity of PCI procedure and the used antithrombotic treatment.
Methods 1895 consecutive patients undergoing PCI with bioabsorbable polymer drug eluting stent were screened for eligibility. Major adverse cardiovascular events (MACE) were defined as composite of death, myocardial infarction, stroke, and unplanned revascularization. Complex PCI was defined as two stents bifurcation strategy, 3 treated vessels, or > 3 stents implanted in the same procedure as previously described.3 Four groups were compared accordingly: Group 1 (dual treatment and complex PCI), Group 2 (dual treatment and non-complex PCI), Group 3 (triple therapy and complex PCI), and Group 4 (triple therapy and non-complex PCI).
Results 256 (13.5%) patients had indication for oral anticoagulation, with 33 excluded patients been commenced on 1–3 months DAPT followed by oral anticoagulation. Mean age was 75 ±9 and 77% male. 40.2% patients had stable angina presentation. Average CHA2DS2-VASc and HAS-BLED scores were 3.7 ±1.3 and 1.7 ±0.7, respectively. In the whole group, one year ischaemic events was 9.4%. There were no differences among four groups in gender, hypertension, smoking history, ejection fraction, the nature of presentation (stable versus acute), CHA2DS2-VASc or HAS-BLED scores. On the other hand, there were significant variations among four groups in terms of age (78 ±7, 76 ±9, 72 ±10, 72 ±10, P= 0.008) and diabetes status (9%, 35%, 29%, 22%, P= 0.036), respectively.
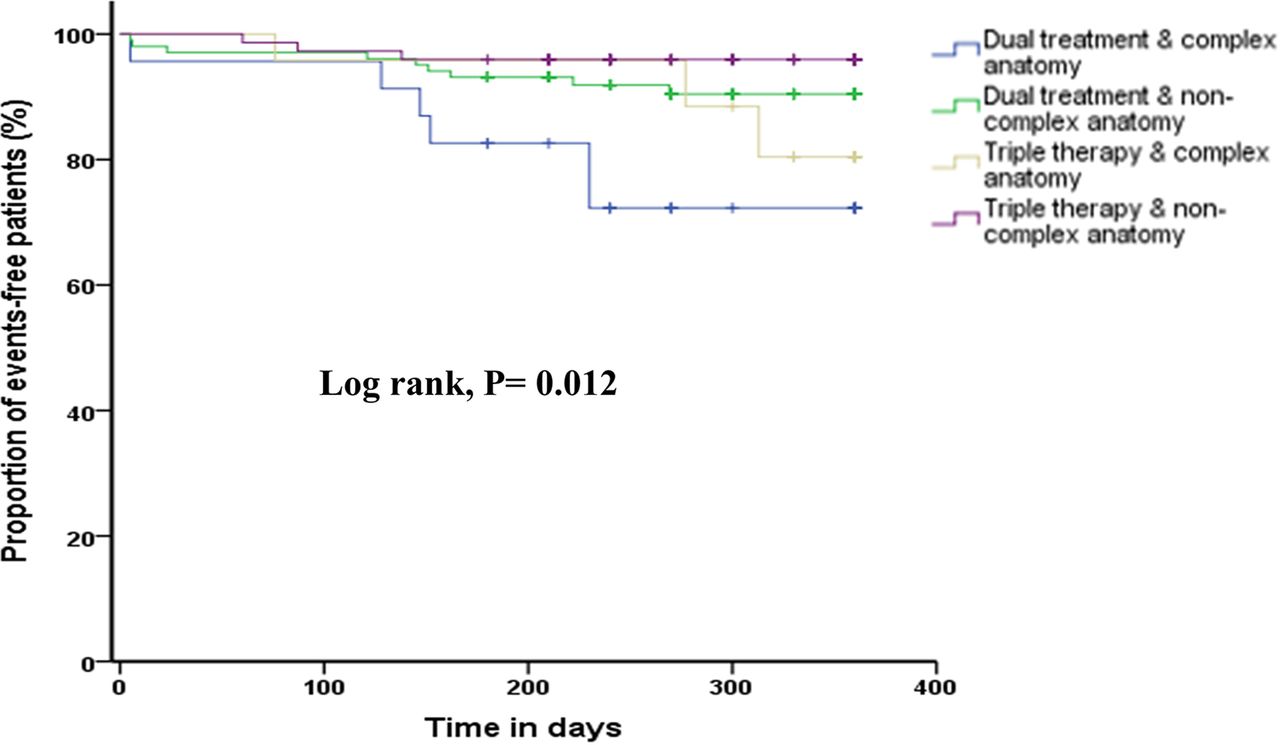
There was a significant difference in the incidence of MACE among four groups, with dual treated-patients and complex anatomy having the highest rate of MACE (26%, 9%, 13%, 4%, Log rank P= 0.012) (figure). The difference was mainly driven from more frequent unplanned revascularisations (13%, 4%, 4%, 0%, P= 0.033) with no difference in death, myocardial infarction or stroke.
Patients with complex anatomy receiving dual treatments had at least 7 times more likelihood of sustaining MACE within the first year following PCI [hazard ratio (HR) 7.36, 95% CI 1.84 to 29.5, P= 0.005]. This risk stayed significant even after adjusting to other variables including age and diabetes status (HR 5.87, 95% CI 1.41 to 24.46, P= 0.015).

{kind=link}
Abstract 160 Figure 1
Conclusion Despite a remarkable low incidence of ischaemic events in patients with AF undergoing PCI using bioabsorbable polymer DES, there is a marked heterogeneity in their future cardiovascular risk. Coronary anatomy and complexity of PCI procedure may play a role in risk stratifying patients with AF to tailor antithrombotic treatment to reduce their risk.
Conflict of Interest None