Article Text

Abstract
Introduction Using fractional flow reserve (FFR) to guide percutaneous coronary intervention (PCI) improves outcomes and reduces costs. In FAME, FFR guidance reduced the total length of stent per patient from 52mm to 38mm and the number from 2.7 to 1.9(1), yet FFR is currently used in <10% of cases (2). Angiography-based virtual (v) FFR solutions permit less invasive physiological assessment and lend themselves to virtual coronary intervention (VCI) (Figure 1). VCI has been shown to predict the response to PCI with a high degree of accuracy(3). In this study, we sought to determine the potential impact of vFFR and VCI on real world stenting.
Methods Patients who had undergone PCI without FFR guidance were identified from the Sheffield archive. A 3D reconstruction of the diseased artery was generated from the angiogram. Baseline vFFR was calculated using computational fluid dynamics (CFD) analysis(4). If vFFR was <0.80, VCI was performed(3). Three PCI strategies were modelled. First, the actual PCI procedure was replicated. Second, the FFRmax was determined; the minimal amount of stenting to achieve the best possible FFR(5). Third, the optimal strategy was determined; the minimal amount of stenting to achieve a post VCI FFR >0.90 (6). For each strategy, the total number and length of stent per patient was determined and compared to the actual procedure, which was conducted in the normal way, guided by the angiogram alone.
Results Forty-three patients (56 vessels) were studied. Mean vFFR pre-PCI was 0.74±0.16.
Twenty-four (43%) vessels had a baseline FFR >0.80. For the actual procedure, mean post-PCI vFFR was 0.90±0.09. The number of stents per patient was 1.4±0.6. Total stent length per patient was 29±15mm. Mean FFRmax was 0.92±0.07. FFRmax was 0.02±0.03 higher than the corresponding measured post-PCI FFR. When the virtual procedure was planned to achieve FFRmax, the number of stents per patient was 0.9±1.0 (p=0.003). Total stent length per patient was 22±27mm (p=0.04). When the virtual procedure was planned to achieve a post VCI FFR >0.90, the number of stents per patient was 0.93±1.02 (p=0.002). Total stent length per patient was 20±25mm (p=0.01).
Conclusion In our cohort, 43% of vessels had a vFFR >0.80 suggesting PCI could have been avoided. Using vFFR and VCI to plan PCI led to a significant reduction in the total number and length of stents recommended per patient. Further work on a larger cohort is required to determine if these findings would translate to improved clinical outcomes.
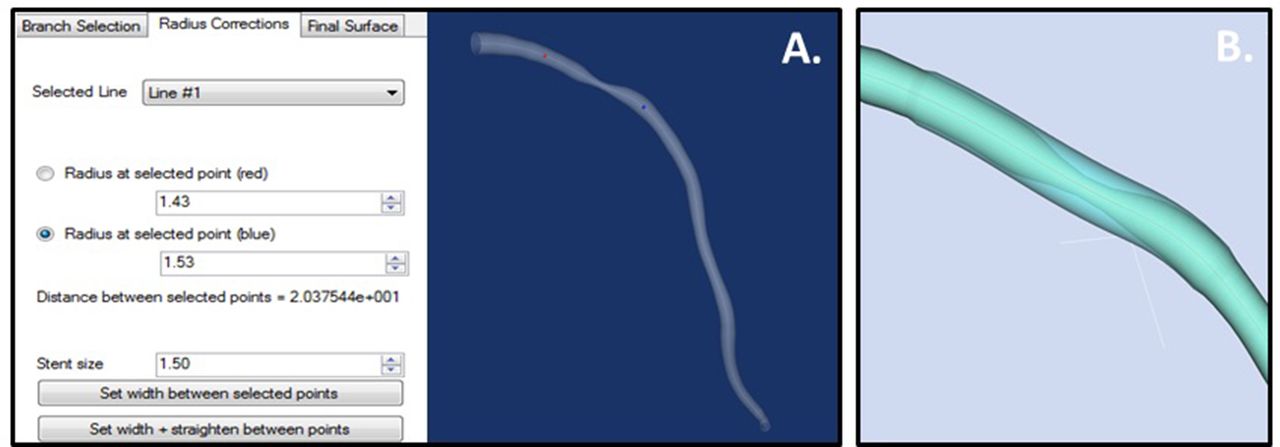
Figure 1: The 3D reconstruction of the artery is displayed and the operator marks the location where they wish to deploy a stent identified by the red and the blue markers (A). The operator can adjust the radius of the desired virtual stent in the box labelled ‘stent size’. The length can be altered by moving the position of the red and blue dots. In the example shown, a 3.0mmx20mm virtual stent has been inserted. The virtually stented artery is shown overlaying the original vessel in panel B. Reproduced from JACC: Cardiovascular Imaging(3) under creative commons license CC BY 4.0
{kind=link}
Abstract 53 Figure 1
Conflict of Interest None