Article Text

Abstract
Introduction Combined positron emission tomography and computed tomography (PET-CT) using the radiotracer 18F-sodium fluoride (18F-NaF) to detect microcalcification provides imaging of both coronary artery anatomy and disease activity simultaneously. While recent studies have suggested that 18F-NaF activity may help identify high-risk coronary atherosclerosis, the role of 18F-NaF uptake in predicting progression of coronary atherosclerosis is unknown. In this study, we aimed to investigate the relationship between baseline coronary arterial 18F-NaF activity and the subsequent progression of coronary arterial calcification in patients with clinically stable coronary artery disease.
Methods Patients with clinically stable, multivessel coronary artery disease underwent combined 18F-NaF PET-CT and CT coronary calcium scoring at baseline with repeat CT coronary calcium scoring at one year. Coronary arterial PET uptake was analysed qualitatively and semi-quantitatively in diseased vessels by measuring maximum tissue-to-background ratio (TBRmax) – defined as the maximum standardised uptake value in a plaque divided by the mean blood pool activity measured in the right atrium. Coronary calcification was quantified by measuring calcium mass (mg), volume (mm3), average calcium density (mg/mm3) and total Agatston score (AU).
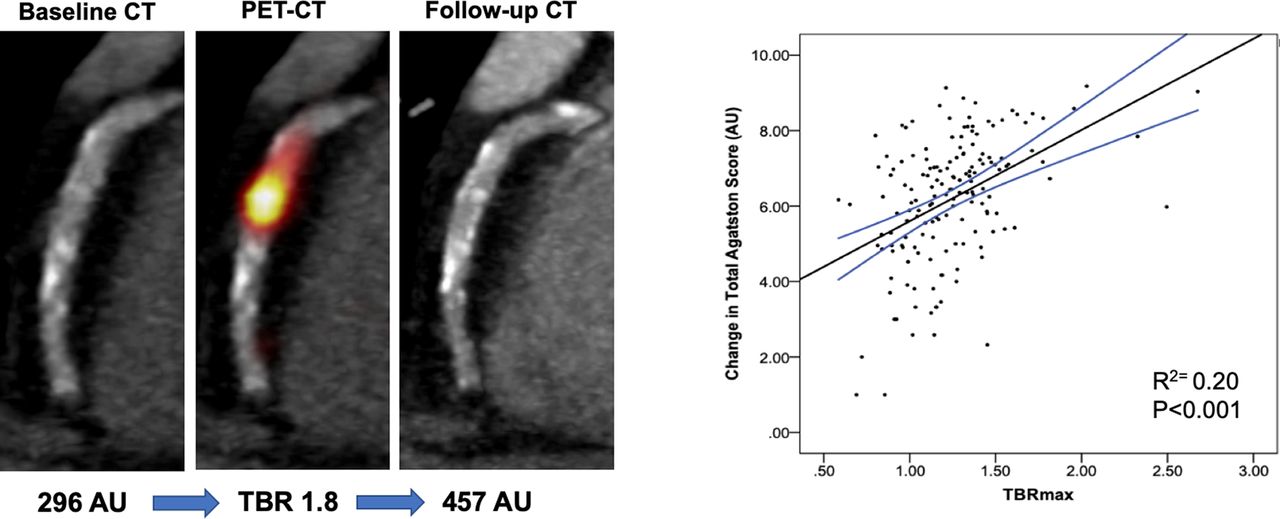
Results One hundred and eighty-three patients who underwent baseline and repeat imaging at one year were included in the study (81% male, median age 66). Of these participants, 116 (63%) had evidence of increased 18F-NaF activity in at least one vessel. Patients with increased 18F-NaF uptake had a higher total calcium score (524[242–1091] AU), volume (491[247–984], mm3) mass (99[46–212] mg) and average calcium density (0.20[0.18–0.23] mg/mm3) at baseline compared to patients without increased uptake (136[55–361] AU, 131[54–343] mm3, 24[11–69] mg, 0.18[0.16–0.20] mg/mm3; P<0.001 for all), and demonstrated greater progression of coronary calcification (table 1). In patients with an increase in calcium score at one year (n=160), there was a moderate correlation between baseline TBRmax and change in total calcium score (R=0.45, R2=0.20; p<0.001) and change in total calcium mass (R=0.50, R2=0.25; p<0.001) at one year (figure 1). There was no correlation between baseline TBRmax and change in average calcium density (p=0.43).
{kind=link}
Abstract 4 Figure 1
Progression of coronary calcification in patients with and without increased 18F-NaF activity at baseline
Conclusion Coronary PET-CT using 18F-NaF identifies patients with a higher calcification burden and predicts progression of coronary arterial calcification at one year.
Conflict of Interest none