Article Text

Abstract
Introduction In the current era of newer generation drug eluting stents, intravascular imaging and potent antiplatelet drugs, percutaneous coronary intervention (PCI) has become an acceptable treatment for left main stem (LMS) disease. Left main stem PCI poses several challenges which can be amplified by the presence of diabetes mellitus (DM). Patients with DM have more extensive and complex coronary artery disease (CAD) with higher rates of stent restenosis and thrombosis. There is a paucity of ‘real world’ outcome data in diabetic patients undergoing LMS PCI.
Our study aims to assess the impact of non-insulin treated (NITDM) and insulin treated (ITDM) diabetes on mortality following LMS PCI. A secondary outcome is to assess mortality in these groups stratified to PCI setting.
Methods We undertook a retrospective analysis of consecutive patients undergoing unprotected LMS PCI between 2004 and 2017 at 2 high volume tertiary centres in the North East of England. The PCI database was interrogated for procedures where at least one vessel treated was the LMS. Ostial LAD and/or circumflex PCI with stenting back to LMS were included. Protected LMS PCI and PCI for iatrogenic dissection were excluded. Diabetic status was recorded as non-diabetic (non-DM), non-insulin treated DM (NITDM) or insulin treated DM (ITDM). The clinical setting for PCI was recorded as ‘elective’ for stable angina, ‘urgent’ for non-ST elevation myocardial infarction and ‘primary’ for ST elevation myocardial infarction.
The primary outcome measure was all-cause 30-day and long term mortality (up to 36 months) post index PCI. Mortality data was provided by the Office of National Statistics and assessed up to 1/10/18.
Results A total of 2702 patients underwent 2778 LMS PCI between 2004 and 2017. Repeat LMS interventions were performed in 76 patients. Twenty-seven patients were excluded as their diabetic status was not known. Of the remaining 2675 patients, 2063 (77.1%) were non-DM, 422 (15.8%) NITDM and 190 (7.1%) ITDM.
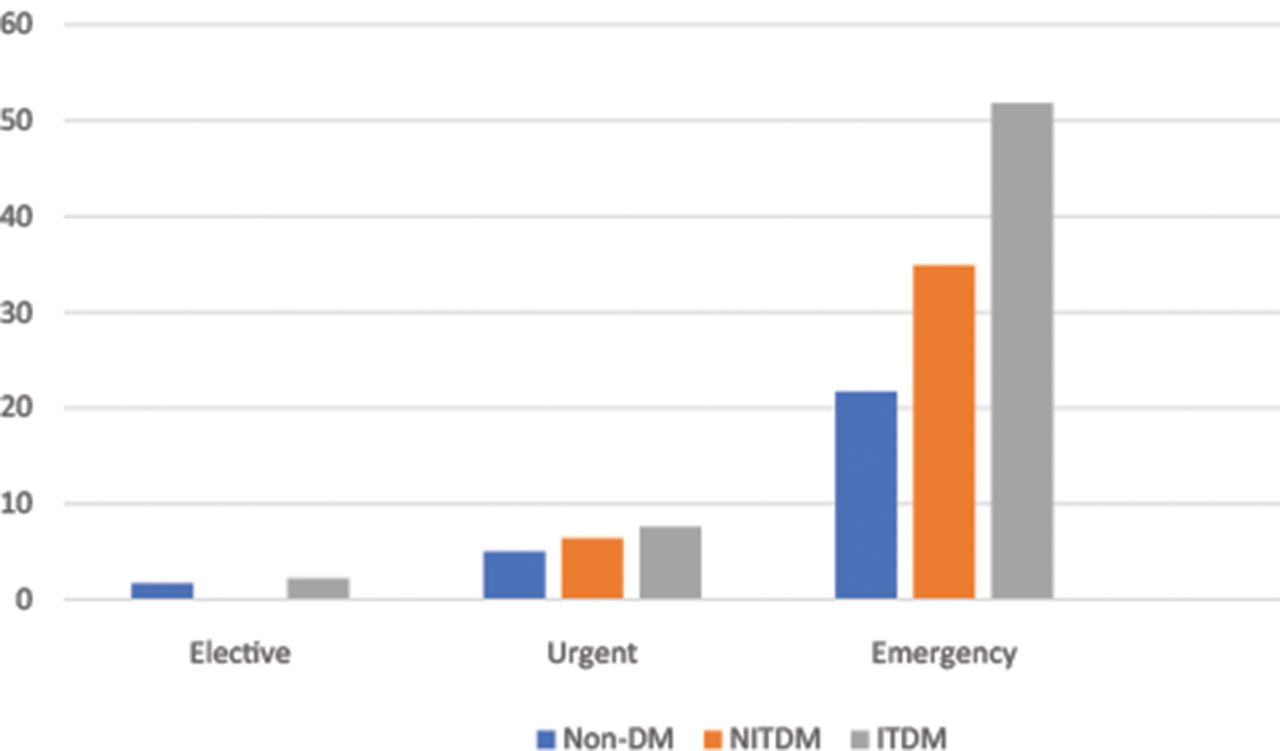
Overall 30-day mortality was 7.8% (figure 1). In a logistic regression model including all LMS PCI, DM status was not associated with 30-day mortality compared to non-DM (table 1). Insulin treated DM but not NITDM was significantly associated with 30-day mortality in the setting of primary PCI (OR 3.54, 95% CI 1.28–9.80, p=0.01).

% Unadjusted 30-day mortality
Abstract 68 Table 1
During a median follow up of 36 months, post 30-day long term mortality was 7.7%. Age, peripheral vascular disease and renal impairment but not diabetes status were associated with long term mortality in all PCI settings (p<0.001). Figure 2 compares the cumulative survival of the DM groups post 30-day follow up using Kaplan-Meier analysis.

{kind=link}
{kind=link}
Survival functions
Conclusion The impact of DM on mortality outcomes following LMS PCI was only significant in insulin treated diabetics following primary PCI. Non-insulin treated DM did not affect short- and long-term mortality when adjusted for other confounders. Our data shows that DM is not an independent predictor of mortality in non-emergency LMS PCI.
Conflict of Interest None