Article Text

Abstract
Introduction Little is known about the variations in atherosclerotic lipid content when juxtaposed to changes LDL-c in response to statin treatment. T2 mapping is a recently-validated magnetic resonance imaging (MRI) technique that can precisely quantify carotid plaque lipid content and its reduction following initiation of high-intensity statin treatment.1 Moreover, this highly-sensitive technique may add insights into the potential differential response of carotid plaque lipid content in ‘normal’ versus ‘abnormal’ carotid arteries.

Abstract 5 Figure 1

{kind=link}
{kind=link}
Abstract 5 Figure 2
Methods Statin-naïve patients presenting with acute myocardial infarction who underwent paired carotid MRI coupled with venous blood sampling were included. Using a modified classification of American Heart Association (AHA) of carotid vessel wall,2 slices of each individual corresponding to type I and II were categorised into the ‘normal’ group while other slices corresponding to type III onward of AHA classification were combined together as the ‘abnormal’ group.
Results 552 patients were included in this study. Mean age was 63 ±13 years and 75% were male. The median EF was 50% (40- 55). 21% of patients were classified as reduced EF, 41% as mrEF, and 38% with preserved EF. There were significant differences across three subgroups (reduced EF, mrEF, and preserved EF respectively) in age (66 ±13, 62 ±13, 62 ±12, P= 0.017), troponin value [4606 (1589- 10000), 2819 (1059- 6347), 902 (329- 2869), (P< 0.001)] and proportion of patients with normal renal function (69%, 82%, 88%, P< 0.001) and anterior STEMI (70%, 45%, 20%, P< 0.001). There was a stepwise increase in the primary endpoint according to the EF category 6.2%, 18.5%, 34.8% P< 0.001 (Figure: Primary endpoint in STEMI patients stratified according to their baseline ejection fraction); hazard ratio (HR) for mrEF versus preserved EF 3.25 (95% CI 1.74 to 6.05), P< 0.001, and HR for mrEF versus reduced EF 0.48 (95% CI 0.31 to 0.74, P= 0.001. The difference was derived from each of the primary components i.e. death (3.3%, 10.1%, 17.4%, P< 0.001), re-admission with heart failure (2.9%, 6.2%, 13%, P= 0.002), and ventricular arrhythmia/ ICD implantation (0%, 4.8%, 12.2%, P< 0.001). There were differential independent predictors of primary endpoint between mrEF and preserved EF (Table 1&2). Normal kidney function was associated with better clinical outcomes in both EF categories.
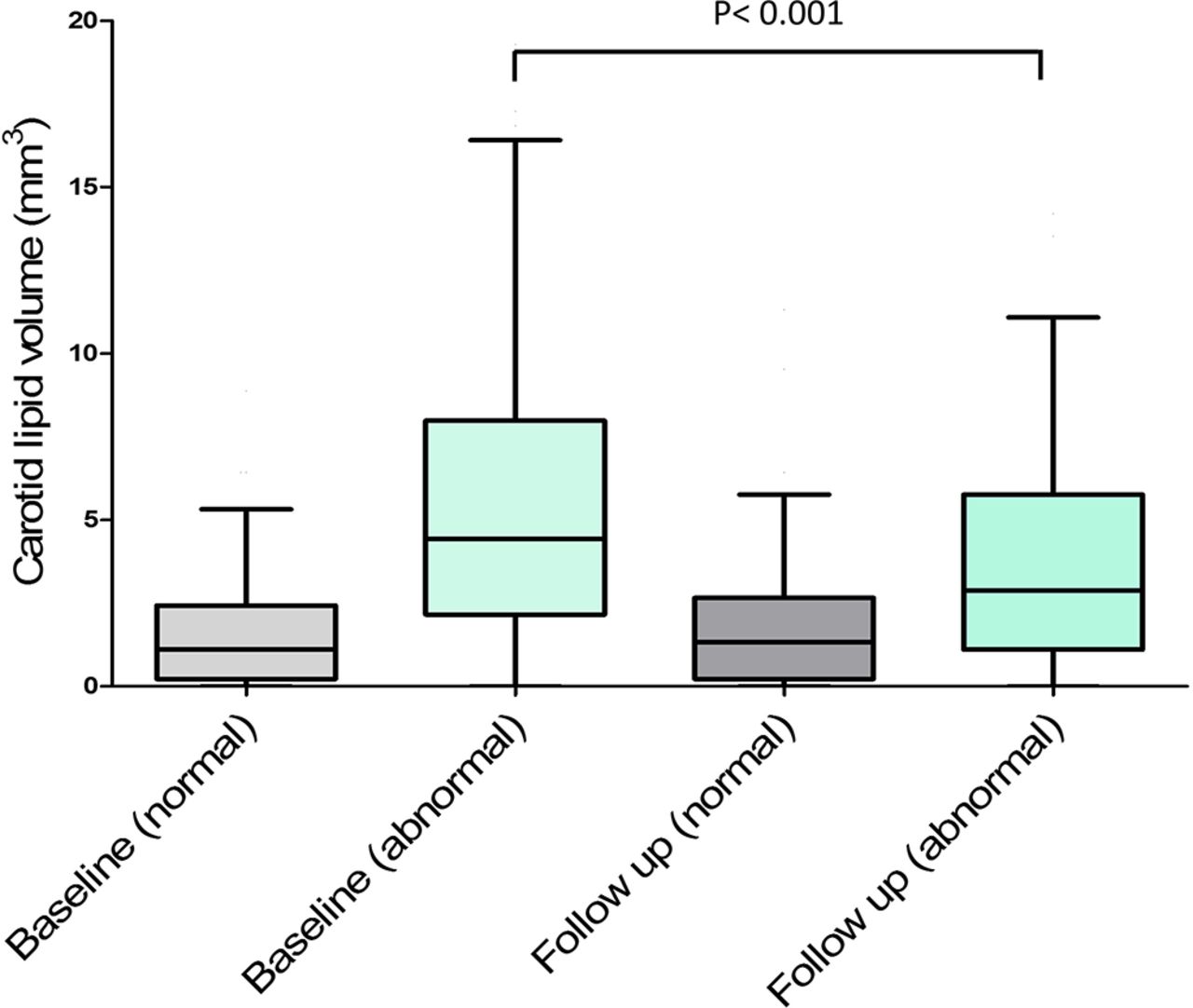
When the cohort was stratified according to the structure of carotid arteries, the group with ‘normal’ carotid slices had no significant changes in carotid lipid% compared to baseline [3.1% (0.5 – 7.1) vs. 3.7% (0.8 – 6.6), P= 0.086]. On the other hand, there was a significant reduction in carotid lipid% in the ‘abnormal’ group when compared to baseline [9.7% (4.1 – 18.4) vs. 6.2% (2.3 – 12.8), P<0.001].
Similarly, there was no significant changes in carotid vessel wall volume after three months of statin treatment in the ‘normal’ group [33.0 mm3 (28.5 – 40.0) vs. 33.3 mm3 (28.8 – 38.6), P= 0.61]. In contrast, a significant reduction in carotid vessel wall volume was detected between baseline and follow up in the ‘abnormal’ group [46.8 mm3 (37.1 – 64.6) vs. 44.6 mm3 (35.0 – 57.7), P<0.001]
Conclusion There was a differential response in plaque lipid reduction between normal and abnormal carotid arteries. Additionally, there was a significant degree of inconsistency in individual response to statin at the level of atherosclerotic plaque lipid content compared with LDL-c. Although LDL-c has a casual role in development of atherosclerosis, other lipid and non-lipid biomarkers have significant impact in determining reduction in atherosclerotic plaque lipid content. Therefore, LDL-c cannot be used, on its own, as a surrogate of plaque lipid reduction. Quantification of plaque lipid content may contribute to the identification of patients at greatest risk of atherosclerosis complications and to the targeting of this group with aggressive lipid lowering drugs.
Conflict of Interest None