Article Text

Abstract
Introduction Coronary artery disease (CAD) remains the leading cause of morbidity and mortality worldwide1. Disability-adjusted life years (DALY) are high in part due to the years of life lost and early onset of disease. Multiple therapeutic interventions including lipid modifying drugs, aggressive blood pressure control, detection and treatment of diabetes and additional lifestyle measures reduce the risk of cardiovascular events in patients with established vascular disease2. Coronary artery calcification (CAC) is initiated and propagated by endothelial dysfunction and vascular inflammation. Thus, the presence of CAC confirms atherosclerotic vascular disease and increases patient risk of adverse cardiovascular events. When identified, primary preventative measures are indicated.
CAC can be detected incidentally on ungated CT chest scans but the finding is often not reported within the standard-of-care radiology report which is focused on the non-cardiac indication for the scan. We sought to retrospectively audit the prevalence of CAC on ungated CT chest imaging in our centre. We examined the patient demographics, history of known vascular disease and prescription of preventative therapies. We also examined the frequency of reporting of this finding.
Method We retrospectively reviewed 200 chest CT scans acquired in the Golden Jubilee National Hospital between 03/09/18 and 01/10/18. Scans were reviewed by two Clinical Teaching Fellows, assessing for CAC using an ordinal scoring method previously described3. The first 50 scans were reviewed by both readers to assess consistency of reporting. Verified radiology reports for each scan were reviewed to record if CAC had been documented.
Demographic information was collected from electronic patient records and the primary care emergency care summary was interrogated to ascertain if the patient was on antiplatelet, anticoagulant or statin therapy.
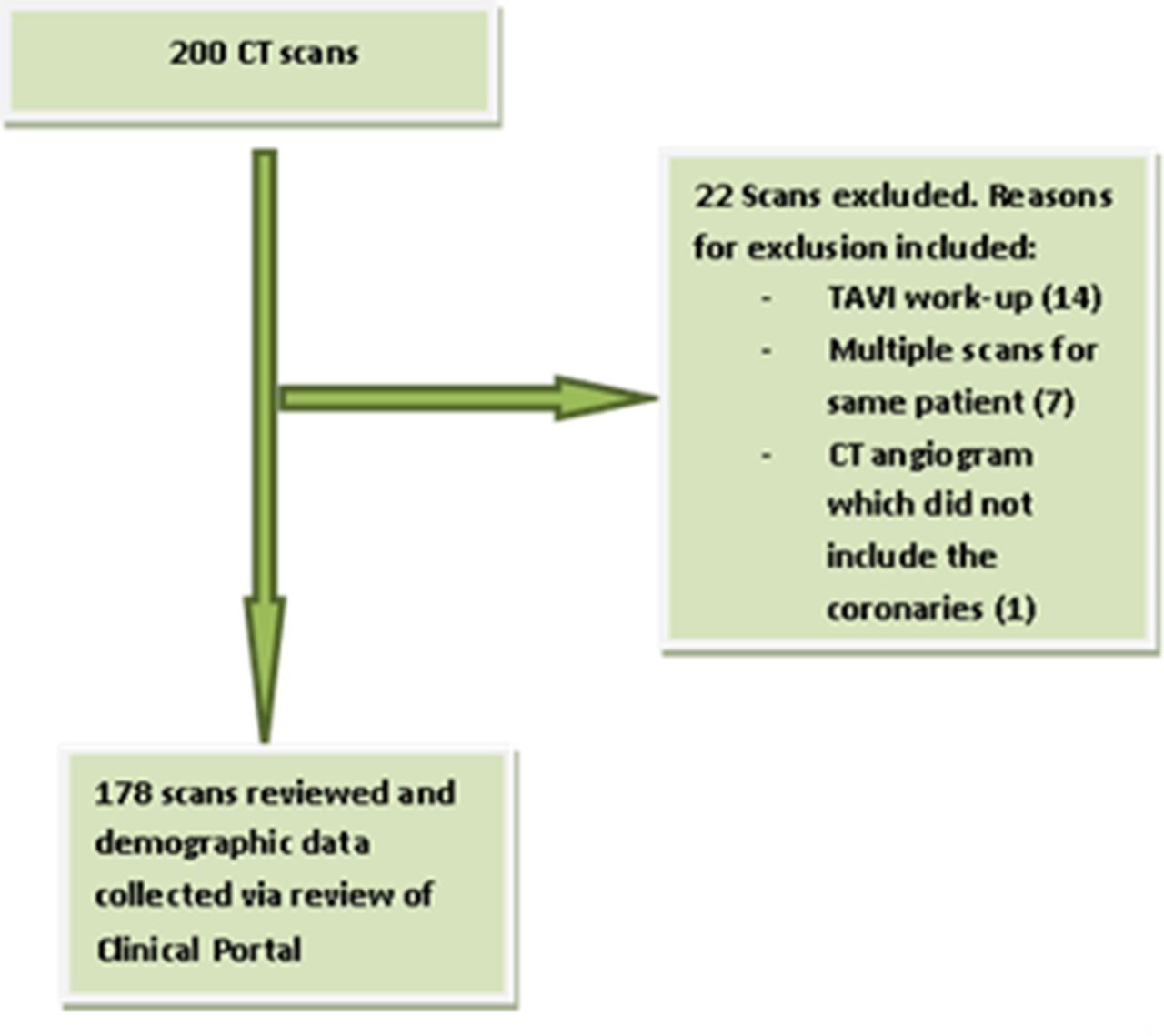
Results 178 scans were suitable for inclusion in the final audit (figure 1). CAC was present on 115 (64%) scans. CAC was reported in 21/115 (18%) scans where it was present. Figure 2 summaries the prevalence of CAC and an established diagnosis of vascular disease (coronary, cerebral or peripheral vascular disease). CAD prevalence was higher with increasing age. Table 1 summarises the risk factor profile for these patients. Data on diagnosis of vascular disease was unavailable for 21 patients. Table 2 shows that only 11 (37%) of 30 patients <65 years and 29 (45%) of 64 ≥65 yrs were prescribed antiplatelet/anticoagulant and statin therapy. Those with no documented vascular disease were less likely to be on treatment with only 4 (19%) of 21 aged <65 yrs and 7 (21%) of 34

Abstract 105 Figure 1
*Clinical portal data unavailable.

{kind=link}
{kind=link}
Abstract 105 Figure 2
Abstract 105 Table 2
≥65 yrs prescribed both preventative therapies.
Conclusion CAC was present on the majority of CT scans but reported in only a minority. Whilst CAC was common in patients ≥65 years only a minority of these patients were receiving guideline-directed preventative therapy. CAC was relatively common in patients aged <65 without a history of vascular disease. This group may have most to gain from early lifestyle and medical intervention prompted by this finding.
Conflict of Interest None