Article Text

Abstract
Objective Tub bathing is considered to have a preventive effect against cardiovascular disease (CVD) by improving haemodynamic function. However, no prospective studies have investigated the long-term effects of tub bathing with regard to CVD risk.
Methods A total of 30 076 participants aged 40–59 years with no history of CVD or cancer were followed up from 1990 to 2009. Participants were classified by bathing frequency: zero to two times/week, three to four times/week and almost every day. The HRs of incident CVD were estimated using Cox proportional hazards models after adjusting for traditional CVD risk factors and selected dietary factors.
Results During 538 373 person-years of follow-up, we documented a total of 2097 incident cases of CVD, comprising 328 coronary heart diseases (CHDs) (275 myocardial infarctions and 53 sudden cardiac deaths) and 1769 strokes (991 cerebral infarctions, 510 intracerebral haemorrhages, 255 subarachnoid haemorrhages and 13 unclassified strokes). The multivariable HRs (95% CIs) for almost daily or every day versus zero to two times/week were 0.72 (0.62 to 0.84, trend p<0.001) for total CVD; 0.65 (0.45 to 0.94, trend p=0.065) for CHD; 0.74 (0.62 to 0.87, trend p=0.005) for total stroke; 0.77 (0.62 to 0.97, trend p=0.467) for cerebral infarction; and 0.54 (0.40 to 0.73, trend p<0.001) for intracerebral haemorrhage. No associations were observed between tub bathing frequency and risk of sudden cardiac death or subarachnoid haemorrhage.
Conclusion The frequency of tub bathing was inversely associated with the risk of CVD among middle-aged Japanese.
- cardiac risk factors and prevention
- acute myocardial infarction
- stroke
Statistics from Altmetric.com
Introductions
Cardiovascular disease (CVD) is the leading cause of premature death worldwide and is associated with individual lifestyle behaviours, such as smoking, physical exercise, drinking and diet.1 2 Bathing is another lifestyle behaviour, and how people bathe differs widely across countries and cultures.
Heat exposure through tub bathing has recently been examined as a potential means of preventing CVD. The impact of heat exposure on diabetes control was first suggested from a report published in 1998, in which eight participants with type 2 diabetes mellitus were asked to bathe in a tub for 30 min a day, 6 days a week for 3 weeks, and were compared before and after the intervention.3 The participants showed a 20% decrease in mean fasting plasma glucose and a 10% decrease in mean glycosylated haemoglobin. Further impacts on blood pressure and weight control were later reported from prospective studies.4 5
Laukkanen et al , employing a 6-year population-based prospective cohort study, showed that sauna bathing was associated with a reduced risk of sudden cardiac death and fatal CVD.6 However, a cardiovascular health benefit of tub bathing has remained to be investigated. Tub bathing provides water pressure that increases stroke volume and cardiac output and reduces total peripheral vascular resistance.7 It is also associated with good sleep quality and self-rated health.8 Conversely, it may be associated with sudden death, particularly in the elderly, by accidental drowning or heart attack triggered by a rapid change in body temperature,9 or by heatstroke in which the increased body temperature cannot be controlled by diaphoresis, while such a risk has not been reported for sauna bathing.6 10
Tub bathing is common in Japan, and frequent tub bathing may be related with Japanese people’s longevity, but no evidence has been available on its long-term effect on risk of CVD. We used a population-based prospective cohort in Japan to investigate the association between tub bathing frequency and risk of myocardial infarction, sudden cardiac death and stroke, and its subtypes in general Japanese population.
Methods
Patient and public involvement
This research was done without patient involvement. Patients were not invited to comment on the study design and were not consulted to develop patient relevant outcomes or to interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
Study population
The Japan Public Health Center-based Study Cohort I is a population-based prospective study of 61 595 Japanese adults aged 40–59 years and from five public health centre areas (Akita, Iwate, Tokyo, Nagano and Okinawa) as per national designation. Excluding the participants from Tokyo, because of the unavailability of incidence data, we used 45 168 participants for the present analyses who were eligible for follow-up. The study design is detailed in a previous article.11 A baseline self-administered questionnaire was distributed in 1990, with 42 840 (94.8%) participants completing a survey including information on tub bathing. In the present study, we also excluded the participants from Okinawa, which is in a subtropical region, as bathing habits in that prefecture differ considerably from in other parts of Japan. Among survey participants from Okinawa, 81.8% bathed in a tub zero to two times per week, and only 10.8% did so almost every day, while these figure 6.4% and 71.9%, respectively, in the other three prefectures. A total of 30 076 participants were subsequently included in the present analysis after excluding a further 1184 who had a history of cancer or CVD at baseline.
Risk factor measurements
Tub bathing frequency was the main exposure of interest. Participants were asked, ‘How often do you bathe in a tub in 1 week?’ and with four possible responses: less than once a week on average, one to two times/week, three to four times/week, or almost daily or every day. As only 0.7% indicated less than once a week on average as a response, we combined the two lowest frequencies as ≤2 times/week.
From the baseline questionnaire, information was also obtained on age at baseline, sex, height, weight, smoking status (never; ex-smoker; or 1–19, 20–29 or ≥30 cigarettes/day), regular physical exercise (rarely or 1–2 or ≥3 times/week), alcohol intake (never; occasionally; or 1–149, 150–299, 300–449 or ≥450 g/week as converted to ethanol), job status (office worker, manual labour worker or not employed), education (junior high school, high school, technical school or junior college, or university or higher), average sleep duration (hours), perceived mental stress (high, medium or low)12 and life enjoyment (high, medium or low).13 Body Mass Index (BMI) was calculated as the reported weight (kg) divided by height squared (m2). Hypertension, diabetes mellitus and hypercholesterolaemia status were determined from responses to baseline questions about the use of medication and the medical history of those respective conditions or diseases. Vegetable (g/day), fruit (g/day),14 fish (g/day)15 and soybean (g/day)16 intakes were assessed using a self-administered food-frequency questionnaire.17
Confirmation of coronary heart disease (CHD) and stroke
Our endpoint was incident CHD or stroke. A total of 17 hospitals contributed to a register of events within the public health centre areas. All were major hospitals with the capability of treating patients with acute CHD, stroke or cancer events. We, therefore, assumed they were able to accurately record most CVD cases. Physicians in the hospitals, public health centres or investigators were blinded to the patients’ lifestyle data and annually reviewed the medical records of cohort participants at the hospitals. They extracted clinical information, including brain images, ECG readings and enzyme levels, which were entered into cohort-specific registration forms.
CHD was defined as myocardial infarction (10th revision of the International Statistical Classification of Diseases and Related Health Problems [ICD-10], I21) or sudden cardiac death (ICD-10, I46.1 and I46.9). Myocardial infarction was confirmed via the medical records by the modified criteria of the Monitoring Trends and Determinants of Cardiovascular Disease project,18 which required self-reported typical chest pain and evidence from cardiac enzymes and ECG. Sudden cardiac death was defined as a death of unknown origin that occurred within 1 hour of event onset.
Stroke was confirmed by the criteria of the National Survey of Stroke,19 which required the presence of focal neurological deficits of sudden or rapid onset and lasting at least 24 hours or until death. Stroke was classified into four subtypes: intracerebral haemorrhage (ICD-10, I61 and I62), subarachnoid haemorrhage (ICD-10, I60), cerebral infarction (ICD-10, I63) or unclassified (ICD-10, I64). For each subtype of stroke, a definite diagnosis was established based on the examination of CT scans, magnetic resonance images or autopsy.
Follow-up
For each participant, we calculated the person-years of follow-up from the baseline to whichever of the following came first: first endpoint, death, emigration or end of the follow-up on 31 December 2009. Changes in residential status were identified through residential registries in each area. Participants who moved out from their original public health centre area were censored at the time of moving.
Statistical analysis
The mean value and prevalence of selected factors were calculated based on tub bathing frequency, and the overall difference across the tub bathing frequency was tested using the multiple linear regression for continuous variables and logistic regression for categorical variables, adjusting for age and sex. The HR and the 95% CI for each outcome were calculated using Cox proportional hazard models using age as the timescale after adjusting for the following potential confounding factors: age at baseline (continuous); sex; BMI; history of hypertension; diabetes mellitus or hypercholesterolaemia; smoking status; regular physical exercise; alcohol intake; job status; education; average sleep duration and perceived mental stress (high, medium or low); life enjoyment (high, medium or low); vegetable (g/day), fruit (g/day), fish (g/day) and soybean (g/day) intakes; and public health centre areas to which the participants belonged. We checked the assumptions of the Cox proportional hazard model and there was no violation of the proportional hazard assumption. We tested statistical interactions for sex by adding to the model a cross-product term for tub bathing frequency (0, 1 and 2) and sex (0 and 1). We conducted analyses pooled across sex (adjusted for sex) because we found no statistical interactions between sex and tub bathing in relation to any cardiovascular outcomes. Also, we tested statistical interactions for subjectively reported water temperature by using a cross-product term for tub bathing frequency (0, 1 and 2) and a categorical variable representing water temperature (0, 1 and 2). In an attempt to reduce potential reverse causation, we also conducted subanalysis after excluding participants who developed CVD or died within 5 or 10 years of baseline. To see the effects of tub bathing on major cardiovascular risk factors, additional analyses were conducted by examining the associations between tub bathing frequency and risks of incident hypertension, diabetes and hypercholesterolaemia during the 5 years among the participants without a history of hypertension (n=26 518), without a history of diabetes (n=29 650) and without a history of hypercholesterolaemia (n=29 442), respectively. We used SAS V.9.4 for the statistical analyses. All statistical tests were two-tailed, with p<0.05 considered as statistically significant.
Results
Table 1 shows the baseline characteristics based on tub bathing frequency. Those who bathed in a tub bath almost daily accounted for the largest proportion of participants at 71.9% (n=21 618). The proportion of women was lower in the ≤2 times/week group than in other groups. Participants who bathed in a tub less frequently were more likely to be current smokers, manual labour workers, not employed, have long sleep duration and a history of diabetes mellitus, but were less likely to be current drinkers, do regular physical exercise, have a higher education and be office workers. Vegetable, fruit and fish intakes tended to be lower among those who bathed in a tub less frequently.
Baseline characteristics based on tub bathing frequency
During 538 373 person-years of follow-up of 30 076 participants, we documented 2097 incident cases of CVD, including 328 CHDs (275 myocardial infarctions and 53 sudden cardiac deaths) and 1769 strokes (991 cerebral infarctions, 510 intracerebral haemorrhage, 255 subarachnoid haemorrhages and 13 unclassified strokes).
Tub bathing frequency was inversely associated with total CVD (the multivariable HR (95% CI) for almost daily or every day versus zero to two times/week=0.72 (0.62 to 0.84), trend p<0.001), total stroke (0.74 (0.62 to 0.87), trend p=0.005) and intracerebral haemorrhage (0.54 (0.40 to 0.73), trend p<0.001), but was not associated with sudden cardiac death or subarachnoid haemorrhage (figure 1 and table 2). Those bathing in a tub ≥3 times/week had a lower risk than those in the ≤2 times/week group for CHD (0.65 (95% CI 0.45 to 0.94), trend p=0.065), myocardial infarction (0.67 (95% CI 0.44 to 1.00), trend p=0.274), and cerebral infarction (0.77 (95% CI 0.62 to 0.97), trend p=0.467), although trend analyses did not reach statistical significance.
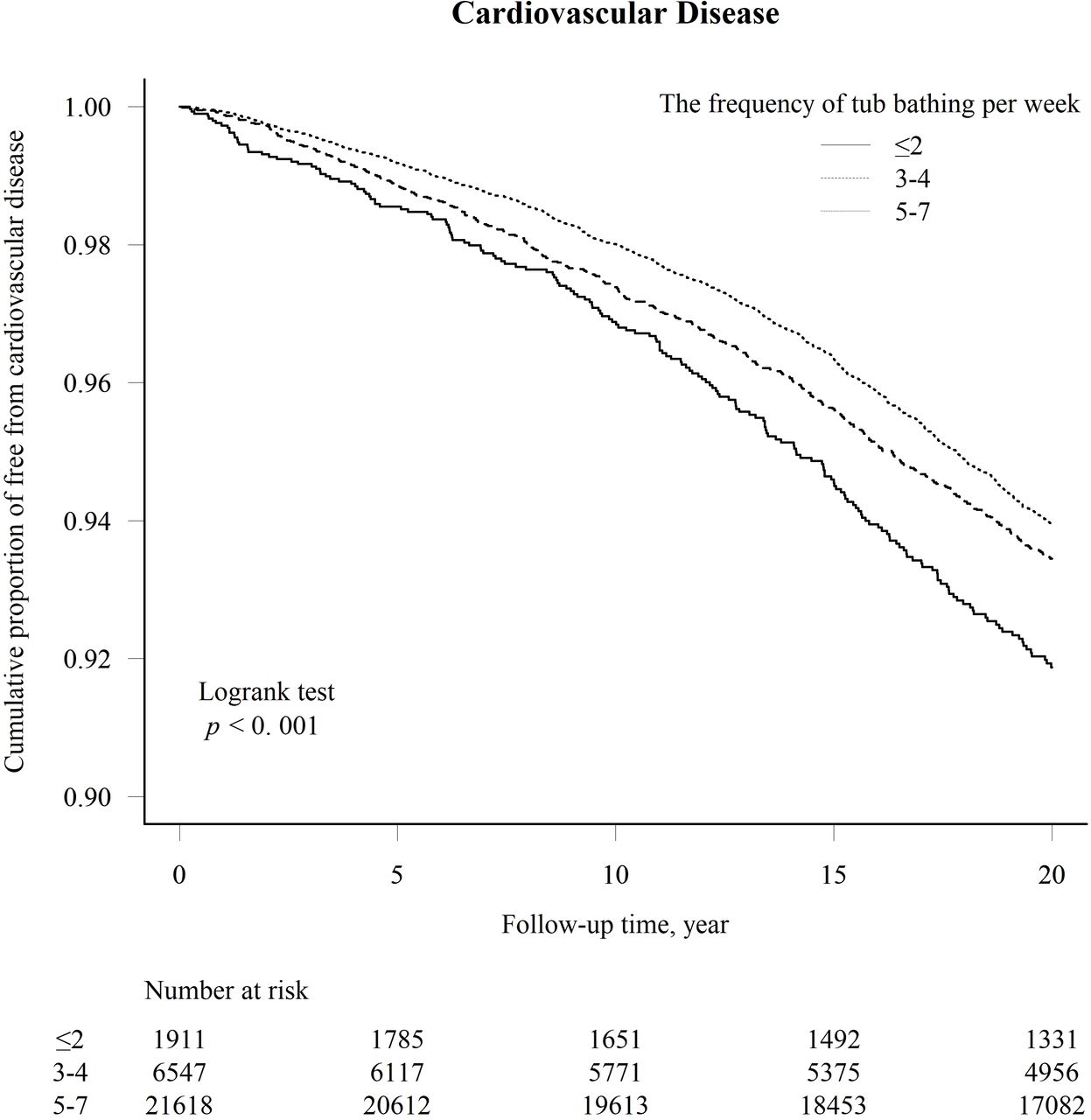
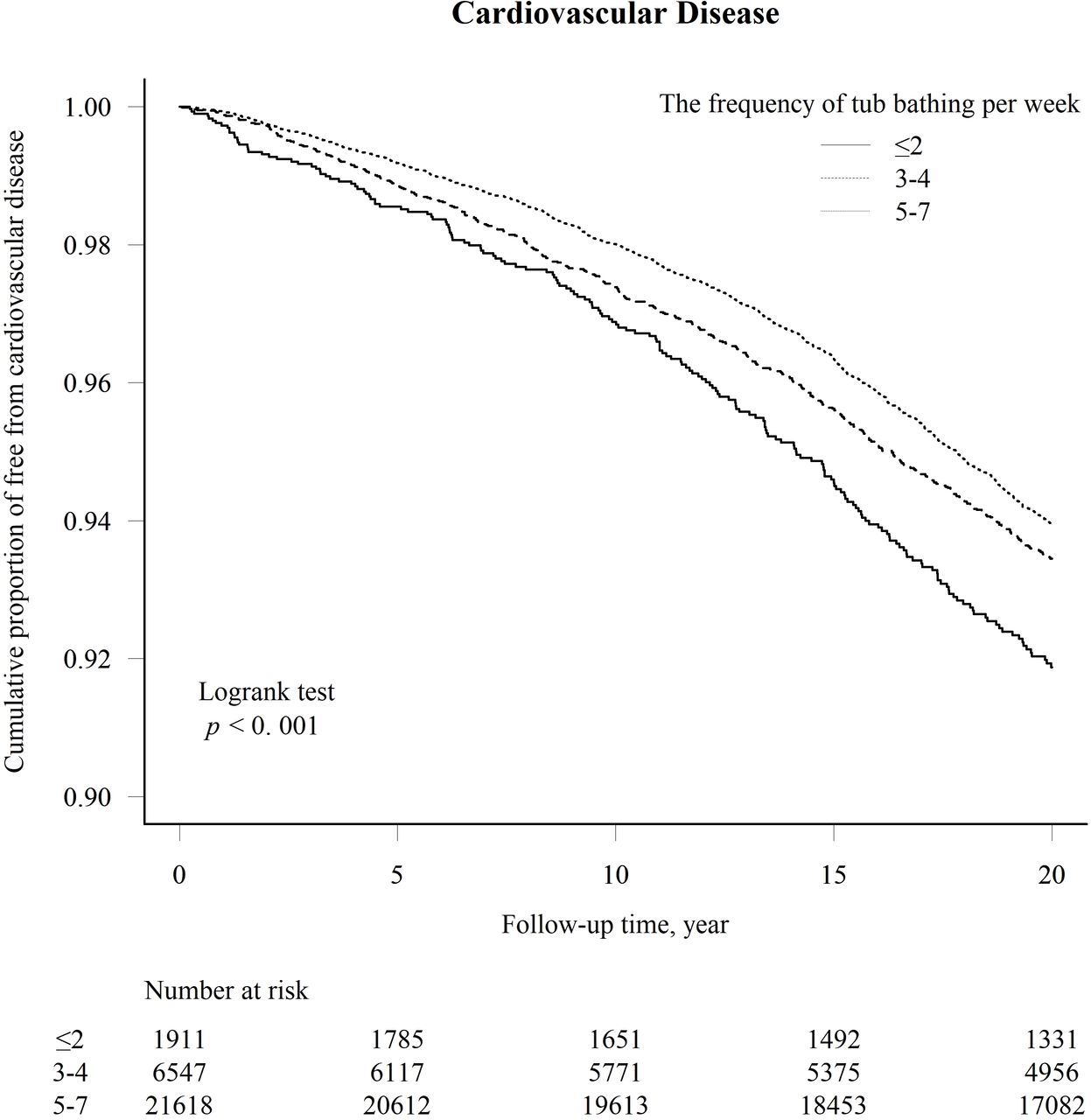{kind=link}
Cumulative Kaplan-Meier curve for proportion of free from cardiovascular disease according to the frequency of tub bathing per week.
HRs and 95% CIs for incident CVD according to tub bathing frequency
Stratifying by tub water temperature, the inverse association between tub bathing frequency and CVD risk, was evident in the warm water group (HR was 0.74 (95% CI 0.61 to 0.90), trend p=0.008) and hot water group (HR 0.65 (95% CI 0.44 to 0.95), trend p=0.056) (table 3). The interaction by temperature was not statistically significant (p for interaction=0.63 for CVD, 0.72 for CHD and 0.88 for total stroke).
Multivariable-adjusted HRs and 95% CIs for incident CVD according to tub bathing frequency after stratification by subjective tub water temperature
After excluding participants who developed CVD within 5 or 10 years of baseline, the inverse associations of total CVD, CHD and total stroke with tub bathing frequency were somewhat weakened but remained statistically significant for total CVD and total stroke (table 4).
Multivariable-adjusted HRs and 95% CIs for incident CVD according to tub bathing frequency after excluding entry incidence within 5 and 10 years from baseline
When examining the association between frequency tub bathing and major cardiovascular risk factors, age-adjusted and sex-adjusted ORs (95% CI) of tub bathing 3–4 times/week, and almost daily or every day in reference to ≤2 times/week were 0.80 (0.65 to 0.98) and 0.80 (0.67 to 0.96) for hypertension, 0.67 (0.42 to 1.05) and 0.71 (0.48 to 1.06) for diabetes, and 1.01 (0.75 to 1.37) and 1.27 (0.97 to 1.67) for hypercholesterolaemia.
Discussion
In the present long-term cohort study of middle-aged Japanese men and women, we observed an inverse association between tub bathing frequency and risks of CVD, CHD, total strokes and intracerebral haemorrhage. Tub bathing was not associated with a higher risk of sudden cardiac death.
This is the first study to examine the long-term associations between tub bathing and CVD incidence using a large population-based cohort. Laukkanen’s study of 2315 men aged 42–60 years in Finland with 6-year follow-up investigated the association of sauna bathing frequency with risks of fatal CVD, fatal CHD and sudden cardiac death. In that study, the multivariable-adjusted HRs (95% CIs) for sauna bathing four to seven times/week compared with one time/week were 0.50 (95% CI 0.33 to 0.77) for fatal CVD, 0.52 (95% CI 0.31 to 0.88) for fatal CHD and 0.37 (95% CI 0.18 to 0.75) for sudden cardiac death.6 However, that study did not examine the effect of sauna on the risk of non-fatal CVD.
A variety of studies have addressed the mechanisms by which heat exposure plays a role in preventing CVD.20 Heat exposure increases core body temperature, cardiac contractility, heart rate and blood flow, and decreases vessel endothelial shear stress.4 21 These effects are similar to the impact of exercise and are believed to improve vascular function over the long term.22 23 Preliminary research found that heat exposure induced expression of heat shock protein 90, and when it was bound to endothelial nitric oxide synthase (eNOS), eNOS, in turn, generated nitric oxide, resulting in vasorelaxation.24 There are, however, physiological differences between tub and sauna bathing; the former increases hydrostatic pressure, which in turn increases intracardiac pressure, while both tub and sauna bathing increase stroke volume, cardiac output, ejection fraction and reduce vascular resistance.25
The potential beneficial effect of tub bathing of CVD events may be mediated by the reduced development of major cardiovascular risk factors in those who took tub bath frequently. We found that the frequent tub bathing was significantly associated with a lower risk of hypertension, suggesting that a beneficial effect of tub bathing on risk of CVD may be in part due to a reduced risk of developing hypertension.
The typical Japanese style of bathing involves filling the tub to shoulder depth with hot water at approximately 40°C–42°C,9 while some prefer temperatures upward of 43°C.26 In two previous controlled trials, one investigated the effects of hot bathing on blood pressure, flow-mediated vascular dilation, arterial compliance and aortic pulse waves among 20 young sedentary adults,4 and the other examined effects on body weight and abdominal circumference among 66 overweight adults.5 Both studies evidenced the favourable effects of tub bathing when using water up to 42°C. The negative aspect of tub bathing is that it can cause heatstroke more frequently when the tub water temperature is too high.27 In our research, we asked participants to subjectively describe their tub water temperature (lukewarm, warm or hot). However, we observed no significant difference in the inverse association between tub bathing frequency and risk of CVD by the water temperature. Our results did not suggest any preferable water temperature, but further research regarding the water temperature is warranted.
We were able to conduct this observational study in a unique culture in which tub bathing is a common habit. The strength of our study included its prospective design, systemic registration of CHD and stroke incidence, use of a large sample from the general population, and a long follow-up duration. The large sample size and long-term follow-up allowed us to perform analysis after excluding participants with early cardiovascular events, and this reduced the possibility of reverse causation.
Nonetheless, several limitations should be acknowledged. First, the information on the tub bathing frequency was obtained only at baseline. Therefore, participants may have changed their frequency during the follow-up period. Second, because those who frequently bathe in a tub were found likely to have higher education and to be office workers, tub bathing frequency may be a behavioural marker for higher socioeconomic conditions. However, the inverse association between tub bathing and risk of CVD outcomes remained statistically significant after adjusting for these socioeconomic variables. Third, we also did not inquire about reasons for bathing in a tub less frequently. For some, this may be due to illness or conditions by which risk of CVD could be elevated. However, the possibility for reverse causation is unlikely, although not totally negated, because the association between tub bathing frequency and risk of total CVD did not change materially after excluding participants who developed CVD or died within 5 or 10 years of baseline. Finally, though we adjusted for potential confounding variables based on previous research, we cannot negate the possibility of residual or unmeasured confounding.
Conclusion
We found that habitual tub bathing was associated with a lower risk of CVD among middle-aged Japanese, suggesting a beneficial effect on the prevention of CVD.
Key questions
What is already known on this subject?
Basic research has shown possible positive effects of tub bathing on cardiovascular disease (CVD) and suggested the mechanism.
What might this study add?
Tub bathing frequency was inversely associated with the risk of CVD shown by a large prospective cohort study. Tub bathing frequency was not associated with sudden death.
How might this impact on clinical practice?
Clinicians could recommend tub bathing to prevent CVD without taking risks of sudden death.
Acknowledgments
We thank all participating staff contributing to the Japan Public Health Center study for their valuable assistance in conducting the baseline survey and follow-up.
References
Supplementary materials
- Press release -
Press release
- Press release -
Footnotes
Contributors TU conceived the idea for the study. TU, HI, KY, IS, YK, HY, IM, NS and ST collated data for the study. TU, HI and ESE analysed the data. TU wrote the first draft. HI, KY, IS, YK, HY, IM, ESE, NS and ST provided revisions to the first draft. All authors approved the final draft.
Funding This work was supported by the National Cancer Center Research and Development Fund (since 2011) and a Grant-in-Aid for Cancer Research from the Ministry of Health, Labour and Welfare of Japan (from 1989 to 2010).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The institutional human ethics review boards of Osaka university and the National cancer center Approved the study. Written informed consent was obtained from participants.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to containing information that could compromise research participant consent.
Linked Articles
- Editorial