Article Text

Abstract
Objective Mitral stenosis increases the risk of atrial fibrillation (AF) and stroke. Large data underlying the trend in incidence, treatment and outcomes of mitral stenosis are lacking.
Methods Based on the Health Insurance Review and Assessment Service database in Republic of Korea, patients who were diagnosed with mitral stenosis between 2007 and 2016 were enrolled. Trends in the incidence rate and changing patterns of treatment and outcome for stroke and systemic embolism and intracranial haemorrhage (ICH) were analysed.
Results A total of 42 075 patients (mean age 60.7±13.5 years, 13 303 (31.6%) male) were included in the present study. The number included 27 824 (66.1%) patients with mitral stenosis and comorbid AF. The age-standardised annual incidence rate per 100 000 of mitral stenosis in Korea decreased remarkably from 10.3 to 3.6 over 10 years. The use of anticoagulation therapy increased consistently. The annual incidence of stroke and systemic embolism showed signs of plateau, while the incidence of ICH increased.
Conclusions The overall incidence rate of mitral stenosis in Korean population has decreased remarkably. As increasing the use of vitamin K antagonist, the annual incidence rate of ICH was increased but the rate of stroke incidence reached a plateau. Alternative effective anticoagulation strategy should be investigated.
- mitral stenosis
- incidence rate
- anticoagulation
- stroke
- systemic embolism
- intracranial haemorrhage
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Mitral stenosis is associated with rheumatic fever, and therefore, it is highly prevalent in low and middle-income countries.1 Studies from Asia reported a prevalence ranging from 0.68 to 11 per 1000.2 3 The incidence of degenerative mitral stenosis in the elderly caused by mitral annular calcification has been on the rise. The incidence and prevalence of mitral stenosis varies among different regions and age groups. No nationwide population-based data were available so far.
Furthermore, the combination of mitral stenosis and atrial fibrillation (AF) increases the risk of stroke more than AF without mitral stenosis.4 Current guidelines recommend anticoagulation with a vitamin K antagonist for patients with rheumatic mitral stenosis and AF or prior embolism.5 The pathogenesis of thrombus formation in mitral stenosis involves blood stasis in the left atrium.4 Therefore, thrombi can form with mild mitral stenosis or even in the absence of AF.6 7 In this regard, thromboembolism associated with mitral stenosis is associated with poor prognosis, suggesting the need for lifelong anticoagulation.8 9 Comprehensive data underlying the natural history, management strategies and outcomes for this group of patients are not available.
In this study, we investigated the trends in incidence, patterns of treatment and clinical outcomes of patients with mitral stenosis based on a nationwide representative database, the Health Insurance Review and Assessment Service (HIRA) of Republic of Korea.
Methods
Data source
Approximately 98% of the overall South Korean population is covered by the universal health coverage system. The HIRA is a national organisation that reviews and assesses medical costs and healthcare service quality, and the claims data of HIRA contain 46 million patients per year. The HIRA database includes data related to diagnosis, treatment, procedures, surgical history and prescription drugs.10 This study used the HIRA database.
Study population
Patients who were diagnosed with any degrees of mitral stenosis between January 2007 and December 2016 were evaluated. New cases of mitral stenosis were screened according to the codes I342, I050 and I052 in the International Classification of Diseases, 10th Revision, and defined if the codes were recorded at least once at hospital discharge or more than twice in the outpatient department. Among these patients, those with mitral stenosis in 2007 were excluded in order to include newly diagnosed cases. Also, the presence of AF was determined in the specific patient population with mitral stenosis. AF was defined by using the code I48. The diagnosis of AF was established similar to mitral stenosis. The patients with surgical mitral valve reconstruction or replacement were excluded from the analyses.
Data collection and study outcomes
We analysed the trends in incidence rate for mitral stenosis and accompanying AF for the period 2008–2016. The prescriptions for antithrombotic therapies including vitamin K antagonist, aspirin, clopidogrel, cilostazol and ticlopidine were reviewed. The incidence rate of ischaemic stroke or systemic embolism after the diagnosis of mitral stenosis was evaluated according to the presence of AF. Ischaemic stroke was defined by the first hospitalisation with a principal diagnosis using the codes I63, I64, I67, I74 and I459. Systemic embolism including renal infarction, splenic infarction, superior mesenteric artery thrombosis and other types of arterial thromboembolism was defined by codes N28, D735, K55 and I74. Also, the incidence of intracranial haemorrhage (ICH), which was defined using the code I61, was evaluated.
Statistical analysis
Baseline characteristics are summarised as the mean±SD for continuous variables and as frequency with percentages for categorical variables. Continuous variables were compared using the t-test and categorical variables compared using either the χ2 test or Fisher’s exact test as appropriate. P for trend was estimated using Cochran-Armitage trend test. P value <0.05 was considered significant. Patients were stratified by sex and 10 years age group, and the rate of age-standardised annual incidence per 100 000 was evaluated. Direct standardisation was performed using South Korean standard population. Statistical analysis was performed using SAS V.9.3 software (SAS Institute).
Results
Clinical characteristics
A total of 42 075 patients who were diagnosed with mitral stenosis were included in the present study between 2008 and 2016. The mean age was 60.7±13.5 years (range, 12–111), and 13 303 (31.6%) were men. Among the patients, 27 824 (66.1%) manifested concomitant AF. Further, 14 675 (34.9%) patients underwent mitral valve surgery. The mean CHA2DS2-VASc score was 4.2±1.8 and 30 344 (72.1%) were treated with vitamin K antagonist. The baseline characteristics of the patients according to the presence of AF are summarised in table 1.
Baseline characteristics of patients with mitral stenosis
Trends in the incidence of mitral stenosis combined with AF
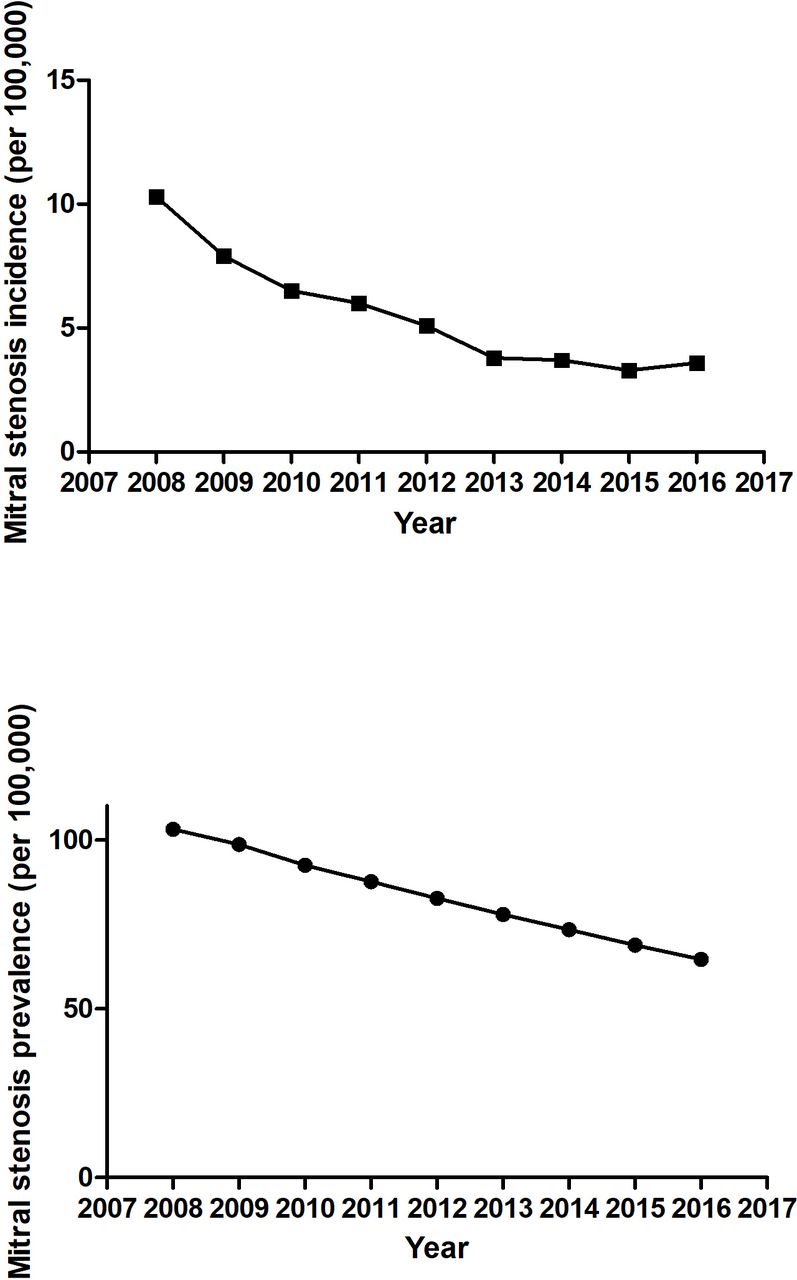
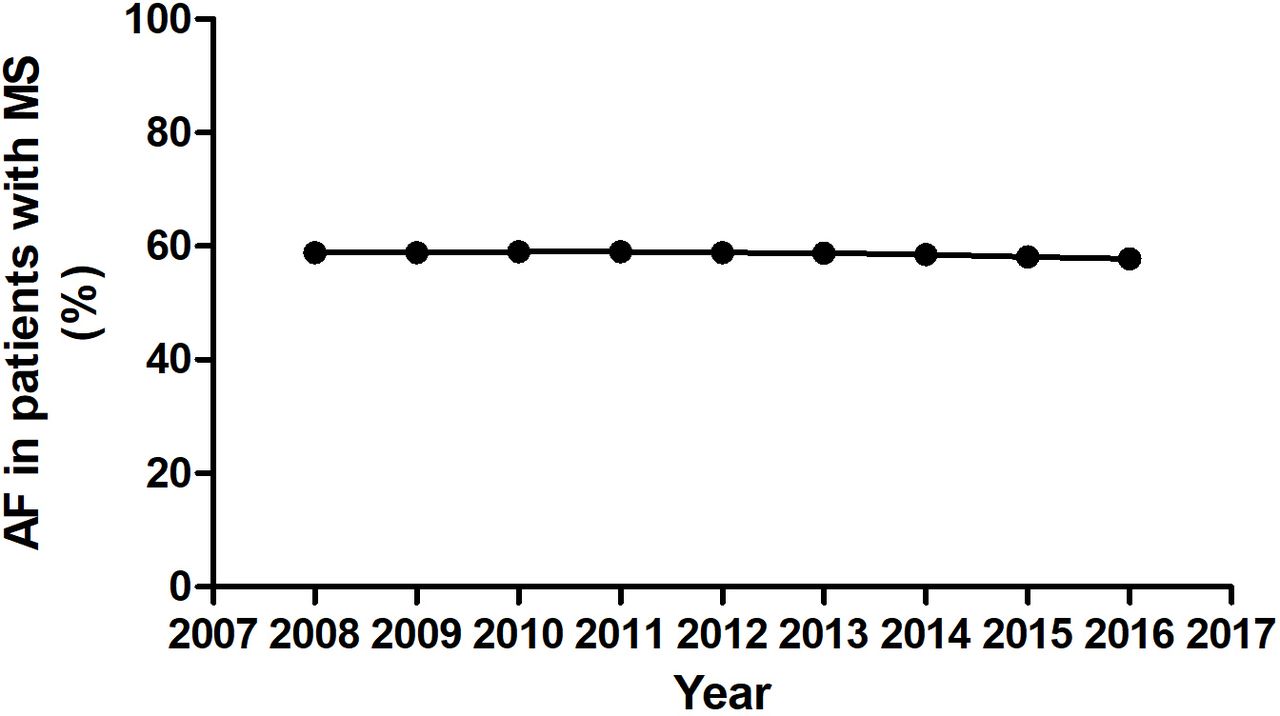
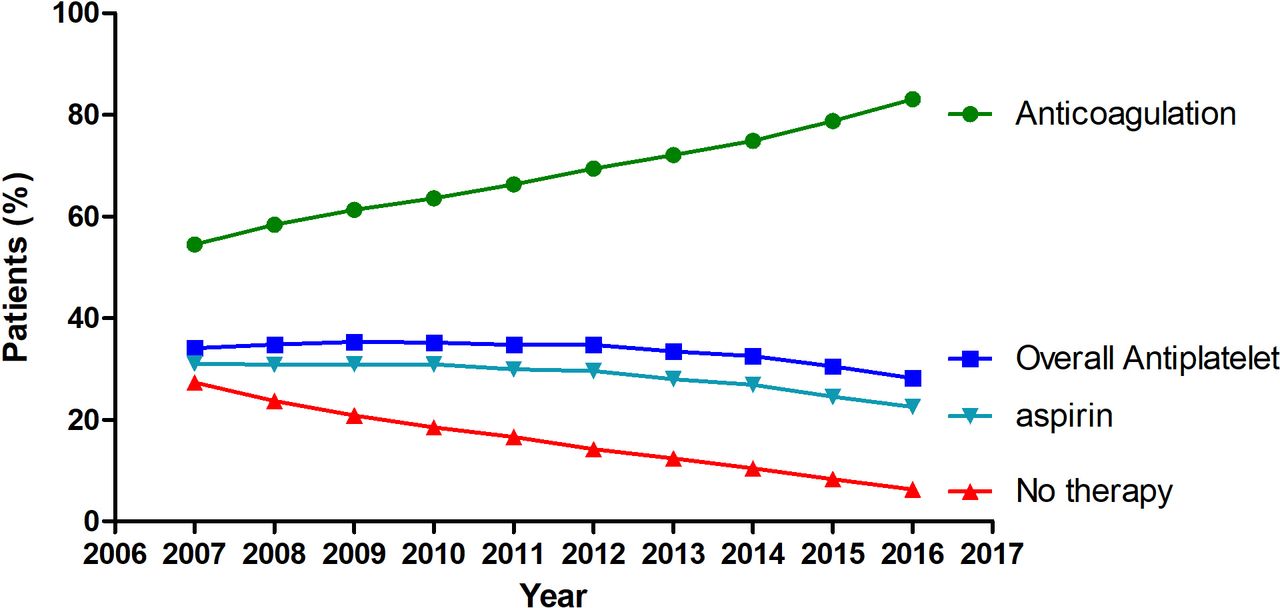
Age-standardised annual incidence rate per 100 000 of mitral stenosis in Korea decreased gradually over time from 10.3 to 3.6 (figure 1). The prevalence rate of AF over time in patients with mitral stenosis showed signs of plateau, constituting approximately more than 60% (figure 2). Antiplatelet agents were prescribed for patients with mitral stenosis and AF up to 34.8% and 28.2% in 2008 and 2016, respectively. The proportion receiving antiplatelet agents was steady over the study period. The use of anticoagulation therapy increased consistently from 58.4% in 2008 to 83.1% in 2016. A detailed proportion of the anticoagulation (warfarin vs non-vitamin K antagonist oral anticoagulant (NOAC)) and drug use according to the sex is given in online supplementary figures S1 and S2. The population who received neither anticoagulation nor antiplatelet agents decreased from 23.7% in 2008 to 6.3% in 2016 (figure 3).
Supplemental material

Age-standardised annual incidence rate per 100 000, prevalence rate for the 2008–2017 period of mitral stenosis in Korea.

Trend showing the prevalence rate of atrial fibrillation (AF) in patients with mitral stenosis (MS).

Trend for antithrombotic therapy for patients with mitral stenosis combined with atrial fibrillation (AF).
Outcome
A total of 6965 (16.5%) patients experienced thromboembolic events and 1606 (3.8%) developed ICH among patients with mitral stenosis with or without AF. The annual incidence of stroke and systemic embolism was significantly higher in patients who manifested mitral stenosis combined with AF compared with mitral stenosis without AF. The incidence rate of ischaemic stroke and systemic embolism was 2.19% in 2008, and 2.26% in 2016 among patients with mitral stenosis combined with AF (p for trend 0.20), while it was 0.26% and 0.31% in patients with mitral stenosis without AF (figure 4). The rate of ICH incidence was less than 1%, however, which showed a tendency to increase over time in patients with mitral stenosis and AF (0.43% in 2008 and 0.72% in 2016, p for trend <0.0001). However, in patients who had mitral stenosis without AF, the incidence rate of ICH was 0.16% in 2008 and 0.09% in 2016 (figure 4, online supplementary figure S3). The incidence rates of all-cause death showed 1.69% in 2008 and 3.94% in 2015 in patients with mitral stenosis combined with AF. In patients who had mitral stenosis without AF, the incidence rate of all-cause death was 1.46% in 2008 and 2.24% in 2015.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Annual incidence rate of outcome for all the patients diagnosed with mitral stenosis with and without atrial fibrillation (AF). ICH, intracranial haemorrhage.
Discussion
This study was the largest investigation into the long-term natural history of mitral stenosis in South Korea. The main findings are as follows. First, we found a significant decrease in the incidence and prevalence of mitral stenosis. Second, the prevalence rate of AF in patients with mitral stenosis exceeded 60%. Third, the proportion of anticoagulation therapy increased steadily over the period. Nevertheless, significant numbers of patients experienced thromboembolic events and the incidence rate of ICH increased.
Trends in mitral stenosis and AF
Mitral stenosis is mostly prevalent in low and middle-income countries due to rheumatic fever.11 Following rheumatic fever, progressive inflammation and injury to the valve contributes to leaflet thickening, commissural fusion and narrowing of the valve. Mitral stenosis is also seen in developed countries under degenerative conditions. The mitral annular calcification is a characteristic feature of degenerative mitral stenosis, which is often seen in elderly or dialysis patients.1 The data presented here suggested a significant decrease in the annual incidence rate of mitral stenosis in South Korea over time and a relative plateau since 2013. Although we could not classify according to the aetiology, our results suggest a decline in the incidence of rheumatic mitral stenosis. Also, the plateau phase indicates development of degenerative mitral stenosis with an increase in the elderly population.
Mitral stenosis remains a major cause of morbidity and mortality, primarily due to the accompanying AF. Mitral stenosis combined with AF is common, and over 20% of patients experience worse outcomes associated with systemic embolism.12 Atrial contraction ensures blood flow across the left atrium to ventricle. The lack of atrial contraction in AF is related to blood stasis in the left atrium, which increases the risk of thrombus formation and also causes dyspnoea.1 Our data showed that almost 60% of patients were diagnosed with a combination with mitral stenosis and AF during long-term follow-up. Mitral stenosis causes atriopathy with atrial inflammation and fibrosis, which leads to AF.
Morbidity
Mitral stenosis induces severe morbidity, including thromboembolism, haemorrhagic transformation, heart failure and death. Death associated with mitral stenosis is mostly caused by systemic embolism or heart failure. As mentioned above, most cases of mitral stenosis show AF, which reduces cardiac output and triggers dyspnoea.1 Also, the risk of thromboembolic events is amplified in the presence of AF.13 Our findings showed a significantly higher incidence of stroke and haemorrhage in patients who manifested mitral stenosis combined with AF compared with mitral stenosis without AF. A recent European cohort study reported similar results, which was a large-scale study of AF and valvular heart disease. Among the native valvular disease, AF with mitral stenosis and aortic stenosis showed greatest thromboembolic risk, yet patients are undertreated with oral anticoagulation.14 Also, our data showed a tendency to increase the all-cause death with this composite morbidity including heart failure, thromboembolism and ICH. The increase of all-cause death could be an increase in the number of elderly patients.
Anticoagulation therapy for patients with mitral stenosis
Thromboembolic risk of mitral stenosis is as high as the risk of prosthetic valve thrombosis.14 Therefore, anticoagulation is mandatory for patients with mitral stenosis combined with AF. All the pivotal clinical trials related to NOAC excluded patients with mechanical heart valves or moderate to severe mitral stenosis.15–18 Therefore, vitamin K antagonist is the only drug of choice to prevent thromboembolic events in patients with mitral stenosis until now. However, the main mechanism of thrombus formation in patients with native valve mitral stenosis is different with prosthetic heart valve. Recently, we reported the efficacy of NOAC in patients with mitral stenosis, although further prospective randomised trials are needed to confirm the usefulness of NOAC in patients with mitral stenosis.19
Guidelines for anticoagulation for AF in patients with mitral stenosis recommend vitamin K antagonist regardless of CHA2DS2-VASc score.5 Our data suggest that anticoagulation therapy is increased gradually in patients with mitral stenosis combined with AF, suggesting the growing physician awareness regarding the need for anticoagulation in patients with mitral stenosis. Our results show that as the proportion of anticoagulation increased, the incidence of stroke did not differ; however, the incidence of ICH tended to increase. Most patients with mitral stenosis have been prescribed warfarin since NOAC is contraindicated for management of mitral stenosis. Warfarin treatment requires maintenance of a proper therapeutic range. The real-world data of the quality of warfarin therapy in Korean patients showed that only 31% of patients were within the therapeutic range.20 Furthermore, a substantially higher incidence rate of ICH with warfarin in the Asian population (HR 4.06, vs Caucasian)21 is already established. In this regard, if NOAC becomes available, it is expected to reduce the risk of thromboembolism as well as the risk of ICH.
Limitation
A major limitation of this retrospective observational study was that it was conducted using claimed data. Therefore, it is difficult to understand the valve characteristics, rheumatic or degenerative. Also, we were not able to ascertain the severity of stenosis. Second, we could not provide the international normalised ratio and time in therapeutic range data because of limitation of claimed national database. Third, we could not analyse the drug combination therapy according to the antiplatelet or anticoagulation agents or stroke rates according to the drug therapy. This might have affected the incidence of ICH or stroke. However, our results present a decade of long-term follow-up observations. Further, thromboembolism or heart failure may have developed even in mild mitral stenosis. Mitral stenosis is a rare disease, and it is hard to observe such a large population. It is meaningful to observe the natural course of the disease in a large population over a long-term period.
Conclusion
This study revealed valuable data underlying the natural history of mitral stenosis. The overall incidence rate of mitral stenosis is decreasing in Korean population and physician awareness of anticoagulation therapy has increased remarkably. Nonetheless, the annual rate of stroke incidence reached a plateau and the incidence of ICH tended to increase. Alternative effective anticoagulation therapy, such as NOAC, should be considered as an important treatment intervention indicated for all such cases.
Key questions
What is already known on this subject?
Mitral stenosis is associated with rheumatic fever, which is highly prevalent in low and middle-income countries.
Also, mitral stenosis increases the risk of atrial fibrillation and stroke.
What might this study add?
Large data underlying the trend in incidence, treatment and outcomes of mitral stenosis are lacking.
The overall incidence rate of mitral stenosis in Korean population has decreased remarkably. The use of anticoagulation therapy increased consistently. The annual incidence of stroke and systemic embolism showed signs of plateau, while the incidence of intracranial haemorrhage increased.
How might this impact on clinical practice?
Physician awareness of anticoagulation therapy in patients with mitral stenosis should be increased.
Also, effective anticoagulation should be needed for efficacy and safety. Alternative effective anticoagulation therapy, such as non-vitamin K antagonist oral anticoagulant, should be considered.
Acknowledgments
The authors acknowledge the financial support of the Catholic Medical Center Research Foundation given in the programme year of 2015.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Funding This study was funded by Catholic Medical Center Research Foundation.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.