Article Text

Abstract
Contemporary Outcomes after Surgery and Medical Treatment in Patients with Severe Aortic Stenosis (CURRENT AS) registry was a large Japanese multicentre retrospective registry of consecutive patients with severe aortic stenosis (AS) before introduction of transcatheter aortic valve implantation. We sought to overview the data from the CURRENT AS registry to discuss the three major contemporary issues related to clinical practice in patients with severe AS: (1) under-referral/underuse of surgical aortic valve replacement (SAVR) in symptomatic patients with severe AS, (2) management of asymptomatic patients with severe AS and (3) management of patients with low-gradient severe aortic stenosis (LG-AS). First, despite the dismal prognosis of symptomatic patients with severe AS, SAVR, including those performed during follow-up, was reported to be underused. In the CURRENT AS registry, overall 53% of symptomatic patients underwent aortic valve replacement (AVR) during follow-up. Second, we reported that compared with conservative strategy, initial AVR strategy was associated with lower risk of all-cause death and heart failure hospitalisation in asymptomatic patients with severe AS. Although current recommendations for AVR are mainly dependent on the patient symptoms, some patients may not complain of any symptom because of their sedentary lifestyle. We also reported several important objective factors associated with worse clinical outcomes in asymptomatic patients with severe AS for risk stratification. Finally, initial AVR strategy was associated with better long-term clinical outcomes than conservative strategy in both patients with high-gradient AS and patients with LG-AS. The favourable effect of initial AVR strategy was also seen in patients with LG-AS with left ventricular ejection fraction of ≥50%.
- transcatheter valve interventions
- aortic stenosis
- valve disease surgery
Statistics from Altmetric.com
Aortic stenosis (AS) is a slowly progressive disease but is associated with dismal outcomes within a few years after symptom emergence if not treated with aortic valve replacement (AVR).1 2 Surgical aortic valve replacement (SAVR) had been the only effective treatment for severe AS for many years.3 However, transcatheter aortic valve implantation (TAVI) has emerged as an effective alternative to SAVR, demonstrating short-term and mid-term outcomes comparable or even superior to SAVR regardless of the surgical risk of the patients.4–7
There still remain three major issues to be discussed related to the clinical practice in patients with severe AS: (1) under-referral/underuse of SAVR in symptomatic patients with severe AS, (2) management of asymptomatic patients with severe AS and (3) management of patients with low-gradient severe aortic stenosis (LG-AS). This article reviews these issues mainly based on the data from the Contemporary Outcomes after Surgery and Medical Treatment in Patients with Severe Aortic Stenosis (CURRENT AS) registry, which was a large Japanese multicentre retrospective registry of consecutive patients with severe AS before introduction of TAVI. We also discuss the current and future clinical practice related to these issues, because the introduction of TAVI has already had substantially changed the management of patients with severe AS.
CURRENT AS registry
CURRENT AS registry is a multicentre, retrospective registry enrolling consecutive patients with severe AS among 27 centres (on-site surgical facility in 20 centres) in Japan between 2003 and 2011 (online supplementary appendix). The design and patient enrolment were previously reported in detail.8 Briefly, we searched the hospital database of transthoracic echocardiography and enrolled consecutive patients who met the definition of severe AS (peak aortic jet velocity (Vmax)>4.0 m/s, mean aortic pressure gradient (PG)>40 mm Hg or aortic valve area (AVA)<1.0 cm2) for the first time during the study period.2 3 We excluded those patients with previous aortic valve intervention.
Supplemental material
Among 3815 patients enrolled in the registry, there were 2005 patients with and 1808 patients without AS-related symptoms at the time of index echocardiography, excluding two patients whose symptomatic status was not available. According to the initial treatment strategies selected after the index echocardiography, 2005 symptomatic patients were subdivided into the initial conservative group (n=1100) and the initial AVR group (n=905), and 1808 asymptomatic patients were also subdivided into the conservative group (n=1517) and the initial AVR group (n=291) (figure 1). During the study period, TAVI was not approved in Japan and was conducted only in the pivotal clinical trial during the follow-up period.

Study flowchart for the CURRENT AS registry. AS, aortic stenosis; AVR, aortic valve replacement; CURRENT AS, Contemporary Outcomes after Surgery and Medical Treatment in Patients with Severe Aortic Stenosis.
Collection of baseline clinical information was conducted via hospital chart or database review. Symptoms related to AS were classified into angina, syncope, chronic exertional dyspnoea or acute heart failure (AHF) requiring hospitalisation. Follow-up data were mainly collected via review of hospital charts; otherwise, data were collected via contact with patients, relatives and/or referring physicians via mail with questions regarding vital status, symptoms and subsequent hospitalisations. Cause of death was classified according to the Valve Academic Research Consortium definitions and adjudicated by a clinical event committee (online supplementary appendix). Follow-up was commenced on the day of the index echocardiography. All patients underwent a comprehensive two-dimensional and Doppler echocardiographic evaluation in each participating centre according to the guidelines.9 Peak and mean aortic PG were obtained with the use of the simplified Bernoulli equation, and AVA was calculated using the standard continuity equation and indexed to body surface area.
Baseline characteristics of the study patients were previously reported in detail.8 10 11 Briefly, among the 3815 patients with severe AS enrolled in this registry, the mean age was 77.8 years, which was much older than in the previous reports,12–15 and 1443 patients (38%) were men. Women were much older than men (79.3±9.6 vs 75.2±9.5 years, p<0.001), and the ratio of women to men increased with age.11 The prevalence of prior myocardial infarction was 8%. The median Society of Thoracic Surgeons (STS) score (predicted risk of mortality) was 3.8% (IQR 2.2–6.6). The Vmax was 4.1±0.9 m/s, and AVA was 0.72±0.18 cm2. There were 405 patients (11%) on maintenance hemodialysis (HD). The median follow-up period of the surviving patients in the entire cohort was 1334 (IQR 1019–1701) days with 93% follow-up rate at 2 years.
Under-referral/underuse of SAVR in symptomatic patients with severe AS
In the CURRENT AS registry, symptomatic patients at baseline were much older and more often had atrial fibrillation or flutter, coronary artery disease or anaemia than asymptomatic patients.10 Surgical risk scores such as logistic EuroSCORE, EuroSCORE II and STS score were significantly higher in symptomatic patients than in asymptomatic patients. Regarding the echocardiographic parameters, symptomatic patients as compared with asymptomatic patients had lower left ventricular ejection fraction (LVEF), larger left ventricular dimensions and higher prevalence of pulmonary hypertension. Symptomatic patients more often had greater AS severity and combined valvular disease such as mitral regurgitation, tricuspid regurgitation and aortic regurgitation, suggesting more advanced stage in extra-aortic valve damage, as recently proposed by Généreux et al.16
Untreated, symptomatic severe AS is known to be associated with a dismal prognosis. Ross and Braunwald proposed a conceptual framework of clinical course of AS in 1968, which was summarised from postmortem studies in adults with isolated AS.17 Once AS-related symptoms emerge, survival becomes poor. The average survival duration after the onset of angina was estimated as 5 years, while the average survival durations after syncope and heart failure (HF) were 3 and 2 years, respectively.17 Despite the dismal natural course of symptomatic patients, SAVR, including those performed during follow-up in previous observational studies, was reported to be underused, ranging from 40% to 70%.15 18–21 The Euro Heart survey showed that 68.2% underwent intervention among patients with severe, symptomatic, single-valve disease, including AS, aortic regurgitation, mitral stenosis and mitral regurgitation.22 In accordance with these reports, only 45% of symptomatic patients were managed with the initial AVR strategy, and overall 53% of symptomatic patients underwent AVR, including those performed during follow-up in the CURRENT AS registry (figure 2). Among 204 asymptomatic patients with class I or class IIa indication for AVR (very severe AS with low surgical risk or severe AS with LVEF<50%), 121 patients (59%) were managed with the initial AVR strategy, and overall 145 patients (71%) actually underwent AVR during follow-up. Previous studies reported advanced age, frailty, the presence of multiple comorbidities or patient rejection as the reasons for non-referral to AVR. In the CURRENT AS registry, symptomatic patients who refused SAVR had less comorbidities and lower STS score but had similarly dismal outcomes as compared with patients who were not referred to AVR due to unacceptably high surgical risk based on the physician judgement. This observation highlighted the profound risk of patient rejection for AVR, as well as the risk of delaying AVR, which the patients and the family members should be adequately informed of.23

Prevalence of AVR in severe symptomatic AS. AS, aortic stenosis; AVR, aortic valve replacement; CAD, coronary artery disease; CURRENT AS, Contemporary Outcomes after Surgery and Medical Treatment in Patients with Severe Aortic Stenosis.
There was no previous large-scale multicentre study assessing the clinical outcomes according to the types of AS-related symptoms in contemporary patients with severe AS. Patients with exertional dyspnoea had significantly higher risk of a composite of aortic valve-related death or HF hospitalisation than those with angina, while the risk of a composite of aortic valve-related death or HF hospitalisation was not significantly different between patients with syncope and those with angina.24 More importantly, management of patients with AHF requiring hospitalisation is particularly challenging. In the CURRENT AS registry, prognosis of patients with severe AS complicated by AHF was poor, with extremely high rates of all-cause death and HF hospitalisation.25 Patients with AHF as compared with patients with chronic HF less frequently underwent AVR and were associated with higher long-term mortality even after AVR. Therefore, careful management to avoid development of AHF would be crucial in patients with severe AS.
TAVI has already transformed the treatment strategies of symptomatic patients with severe AS. In the PARTNER (the Placement of Aortic Transcatheter Valves) randomised trial, TAVI as compared with standard treatment was associated with a relative 44% risk reduction for all-cause death and 59% risk reduction for rehospitalisation at 2-year follow-up in patients with severe AS who were not suitable for SAVR.26 In the real clinical practice, however, conservative management had often been selected in patients with symptomatic severe AS who are at high risk but not suitable for SAVR, while TAVI has often been chosen in this group of patients. Therefore, the magnitude of benefit provided by TAVI as compared with conservative management could not be fully assessed in the PARTNER randomised trial that had enrolled inoperable patients. However, there was no previous study exploring how much clinical benefit could be provided by TAVI in comparison with conservative management in patients with severe AS in the real clinical practice. In a historical comparison between the CURRENT AS registry8 and the Kyoto University-related hospital Transcatheter Aortic Valve Implantation registry,27 TAVI in the early Japanese experience was associated with striking risk reduction for all-cause death (relative risk reduction: 54%), as well as HF hospitalisation (relative risk reduction: 75%), as compared with the historical cohort of patients with severe AS who were managed conservatively just before introduction of TAVI in Japan.28
Management of asymptomatic patients with severe AS
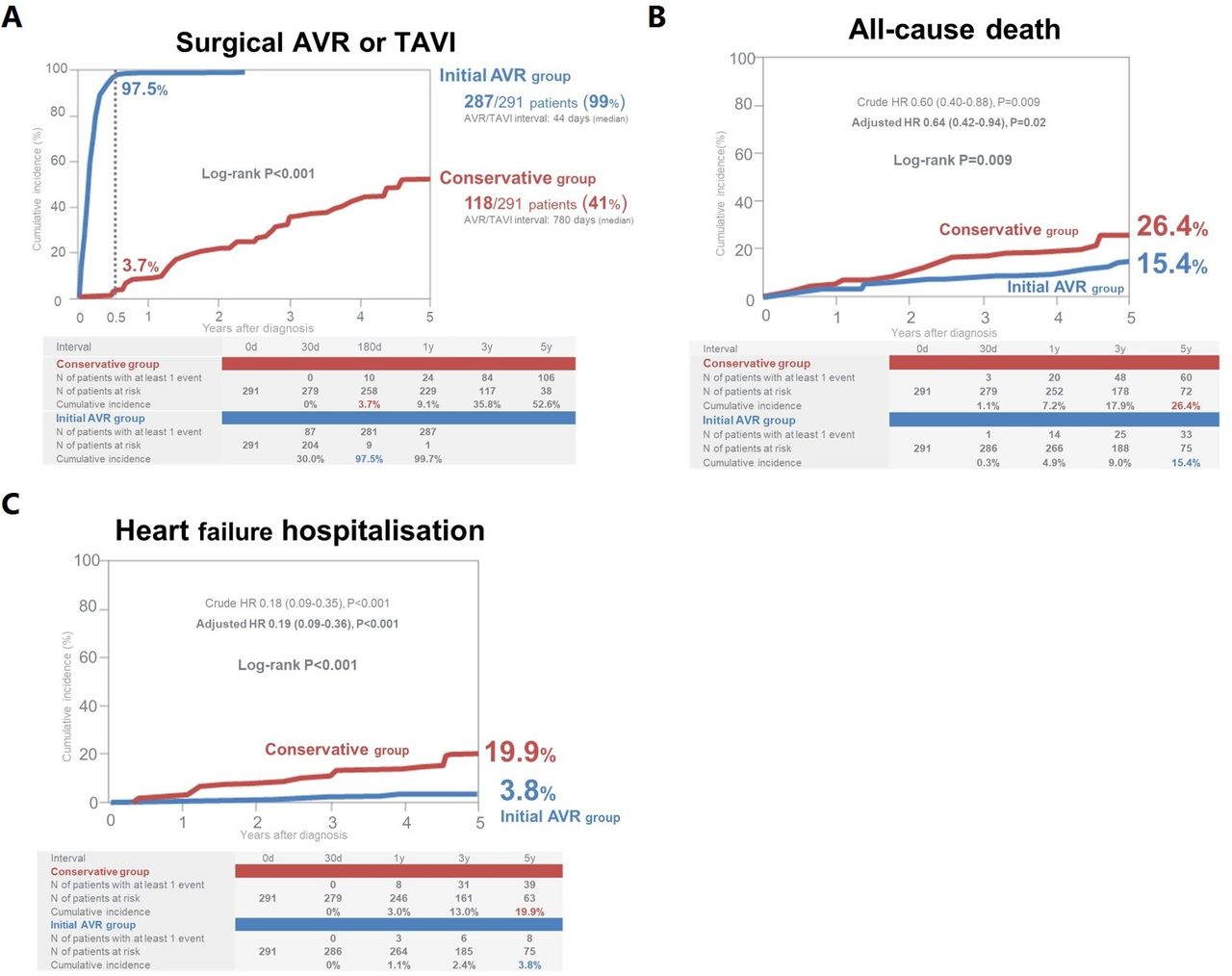
Survival during the asymptomatic phase of AS has been reported to be similar to that of age-matched controls with a low risk of sudden death when patients are followed up closely to report symptoms promptly.12–15 The potential benefits of AVR in asymptomatic patients with severe AS have not been thought to outweigh the operative mortality of AVR.29 Therefore, current guidelines recommend watchful waiting strategy until symptoms emerge for AVR in asymptomatic patients with severe AS except for those asymptomatic patients with very severe AS and/or LVEF<50%, or symptoms on exercise testing.1–3 However, this recommendation was based on previous small single-centre studies12–15 and was supported by a low level of evidence.30 Furthermore, there is no large-scale study comparing an initial AVR strategy with the conservative strategy in asymptomatic patients with severe AS except for one small single-centre observational study in patients with very severe AS.31 In the primary report from the CURRENT AS registry,8 the initial AVR strategy as compared with the conservative strategy was associated with lower risk of all-cause death as well as HF hospitalisation in asymptomatic patients with severe AS in a propensity score-matched analysis (figure 3). Among 291 asymptomatic patients with severe AS in the initial AVR group, 63% of patients had one or more formal indications for AVR, such as very severe AS, LVEF<50%, rapid progression or other cardiac surgery. Among 1517 patients in the conservative group, AVR was performed in 392 patients (cumulative 5-year incidence: 41%) during follow-up with a median interval of 788 days. The cumulative 5-year incidences of all-cause death and HF hospitalisation were significantly lower in the initial AVR group than in the conservative group (15.4% vs 41.7% and 3.8% vs 25.4%, respectively) (figure 3). Several important issues should be considered regarding the clinical relevance of the watchful waiting for AVR strategy. First, the current recommendations for AVR are mainly dependent on the patients’ symptoms. However, many patients with severe AS who could potentially benefit from AVR may not complain of any symptoms because of their sedentary lifestyle. Second, prompt detection of symptoms during follow-up is not always possible in real clinical practice.2 Patients may not always be compliant to the close clinical follow-up.32 In the CURRENT AS registry,8 severe HF was the initial symptom during follow-up in a substantial proportion of patients in the conservative group, in whom AVR was less frequently performed than in patients without severe HF, and mortality was extremely high if AVR was not performed. Third, SAVR after symptom development might be carrying higher operative risk than SAVR during the asymptomatic phase.33 Fourth, the annual rate of sudden death during the asymptomatic phase might be higher (1.4%/year) than the rate (<1.0%/year) reported previously.10 13–15 Finally, in the CURRENT AS registry, 41% of patients managed conservatively required AVR within a median follow-up of 2 years, suggesting that one does not gain much by waiting (figure 4). The biggest limitation of the observational study comparing initial AVR strategy with conservative strategy was the fact that the conservative group had inevitably included those patients ineligible for surgical AVR who were deemed to have very poor prognosis. Nevertheless, a stratified analysis by age in asymptomatic patients with severe AS also demonstrated that the favourable effect of initial AVR relative to conservative strategy for HF hospitalisation was seen not only in patients aged ≥75 years but also in patients aged <75 years, in whom the proportion of those patients ineligible for surgical AVR would have been much smaller than in patients aged ≥75 years.34 Therefore, balancing the risks of the watchful waiting for AVR strategy and the improvement in operative mortality, we found that AVR during the asymptomatic phase might be a viable treatment option in patients with severe AS at low risk for AVR.
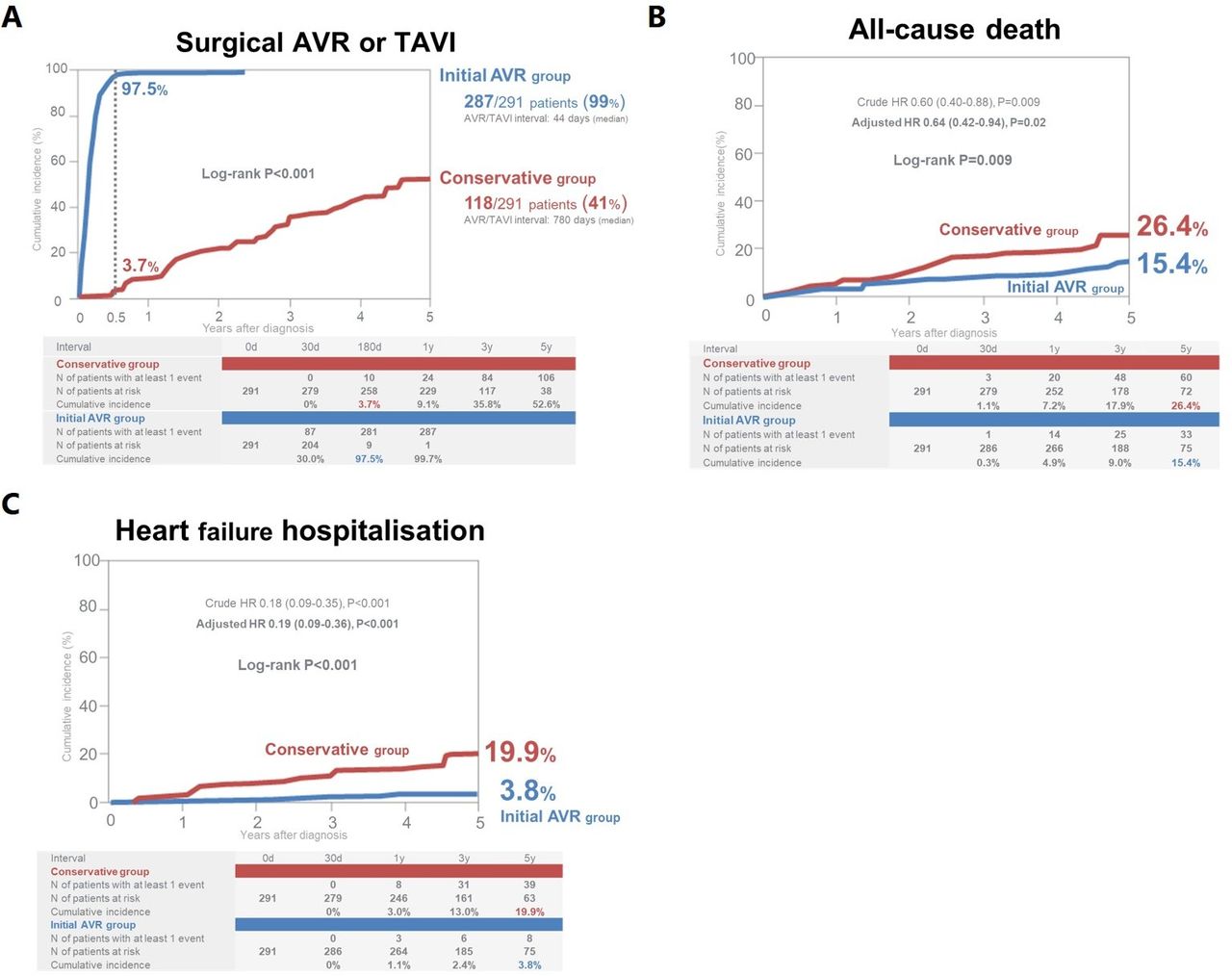
Cumulative incidences of surgical AVR or TAVI (A), all-cause death (B) and heart failure hospitalisation (C) in asymptomatic patients with severe aortic stenosis in the propensity score-matched cohort. Reprinted from Taniguchi et al 8 with permission from Elsevier. AVR, aortic valve replacement; TAVI, transcatheter aortic valve replacement.

Potential reasons for the poor prognosis of asymptomatic patients with severe AS without aortic valve intervention. AVR is indicated in asymptomatic patients with depressed LV function (LVEF<50%) not due to other causes or very severe AS (Vmax≥5.0 m/s or mean aortic PG ≥60 mm Hg) and in patients who develop symptoms during exercise testing. Asymptomatic patients with severe AS should be followed up under active clinical surveillance and should be referred for SAVR or TAVI if some symptoms emerge. However, assessment of symptoms is often difficult in clinical practice, especially in the elderly, leading to false diagnosis of ‘asymptomatic AS’. Furthermore, patients may not always be compliant to close clinical follow-up. Severe HF is often the initial symptom in a sizeable proportion under ‘clinical surveillance’, for whom AVR is less frequently performed than in patients without severe HF, and mortality would be high if AVR is not performed. Operative mortality of SAVR after symptom onset is higher than that in asymptomatic patients. Furthermore, sudden death occurs not infrequently without any preceding symptom in asymptomatic patients with severe AS (1.4%/year). Finally, AVR is anyway inevitable in a short period of time. AS, aortic stenosis; AVA, aortic valve area; AVR, aortic valve replacement; BNP, B-type natriuretic peptide; CURRENT AS, Contemporary Outcomes after Surgery and Medical Treatment in Patients with Severe Aortic Stenosis; ETT, exercise treadmill test; HF, heart failure; LV, left ventricle; LVEF, left ventricle ejection fraction; NYHA, New York Heart Association; PG, pressure gradient; SAVR, surgical aortic valve replacement; TAVI, transcatheter aortic valve replacement; Vmax, peak aortic jet velocity.
In real clinical practice, some risk stratification would be undoubtedly necessary in the triage of asymptomatic patients with severe AS for early AVR. We have reported several important objective factors associated with worse clinical outcomes in asymptomatic patients with severe AS, which might be useful for risk stratification and therapeutic decision-making. First, one of the most important prognostic factors was reported to be LVEF, leading to the recommendation of early AVR in asymptomatic patients with LVEF<50%. Traditionally, systolic left ventricular function is regarded as preserved when LVEF is ≥50%.2 3 In the CURRENT AS registry, LVEF of 50%–59%, as well as LVEF of <50%, but not LVEF of 60%–569%, was independently associated with poorer clinical outcomes compared with LVEF of ≥70%.35 In patients who were managed with the initial AVR strategy, the negative effect of low LVEF was markedly attenuated without any significant difference across the four LVEF groups. Similar results were reported from other recent studies.36–38 Therefore, the cut-off value of the LVEF was raised from 50% to 60% to improve the identification of subclinical LV dysfunction in a recent paper reporting the staging cardiac damage in asymptomatic patients with severe AS.39 We also showed that the patients with a >10% decline of LVEF at the 1-year follow-up echocardiography had a worse clinical outcomes compared with those without decline in LVEF regardless of the baseline LVEF.40 Second, haemodynamic severity of AS is also prognostically important, and Vmax is reported to be a robust prognostic parameter in AS.12 14 15 In the CURRENT AS registry, a greater Vmax (not only Vmax≥5.0 m/s but also Vmax 4.5–5.0 m/s) was associated with incrementally higher risk for a composite of aortic valve-related death or HF hospitalisation in both symptomatic and asymptomatic patients with severe AS.41 Also, AVA≤0.6 cm2 was associated with higher risk of adverse aortic valve-related events compared with AVA>0.80 cm2.42 Third, an inappropriately high LV mass was reported to be a risk factor for mortality in patients with severe AS.43 In the CURRENT AS registry, the LV mass index were independently associated with poorer clinical outcomes in patients with severe AS who were managed conservatively, while its negative prognostic impact was not seen in patients with the initial AVR strategy.44 Fourth, in the European guidelines for the management of severe AS, an elevated B-type natriuretic peptide (BNP) level (more than threefold age-corrected and sex-corrected normal range) without other explanations was a class IIa (level of evidence C) recommendation for surgical AVR in asymptomatic patients with severe AS.3 We confirmed that an increased BNP level was associated with a higher risk of AS-related adverse events in asymptomatic patients with severe AS who were not referred for AVR at the index echocardiography.45 Asymptomatic patients with a BNP level of <100 pg/mL had a relatively low event rate at 1 year of follow-up, who might be safely followed up with watchful waiting strategy. Finally, in the CURRENT AS registry, HD,46 anaemia47 and tricuspid regurgitation48 were associated with poor clinical outcomes in patients with severe AS.
We also proposed a clinical scoring system to predict AS-related events within 1 year in asymptomatic patients with severe AS.49 The risk score comprised independent risk predictors, including LVEF<60%, haemoglobin≤110 g/dL, chronic lung disease (two points), diabetes mellitus, HD and any concomitant valve disease (one point). The predictive accuracy of the model was good with areas under the curve of 0.79 and 0.77 in the derivation and validation sets. Unfortunately, BNP was not included in the clinical scoring system due to the large numbers of missing value for BNP in the CURRENT AS registry. The clinical scoring system might be helpful for decision-making for AVR in the periodic follow-up of asymptomatic patients with severe AS.
The RECOVERY (Randomized Comparison of Early Surgeryversus Conventional Treatment in Very Severe Aortic Stenosis) trial recently reported that the incidence of the primary outcome measures (death during or within 30 days after surgery (operative mortality) or death from cardiovascular causes during the entire follow-up period) was significantly lower among patients who underwent early surgical AVR than among those who were managed conservatively in asymptomatic patients with very severe AS.50 However, this study population included younger patients with less comorbidities and higher prevalence of bicuspid valve than those patients treated in the contemporary clinical practice. Therefore, the definitive conclusions on the role of early AVR in asymptomatic patients with severe AS should be drawn based on the ongoing randomised controlled trials (Aortic Valve Replacement versus Conservative Treatment in Asymptomatic Severe Aortic Stenosis),51 Evaluation of Transcatheter Aortic Valve Replacement Compared to Surveillance for Patients with Asymptomatic Severe Aortic Stenosis, Early Surgery for Patients with Asymptomatic Aortic Stenosis) and Early Valve Replacement Guided by Biomarkers of LV Decompensation in Asymptomatic Patients With Severe AS).
In real clinical practice, many patients with severe AS would not accept the option of early SAVR, if they are truly asymptomatic without limitation of quality of life. Introduction of TAVI in asymptomatic patients would certainly lower the hurdle for them to undergo AVR by TAVI.
Management of patients with LG-AS
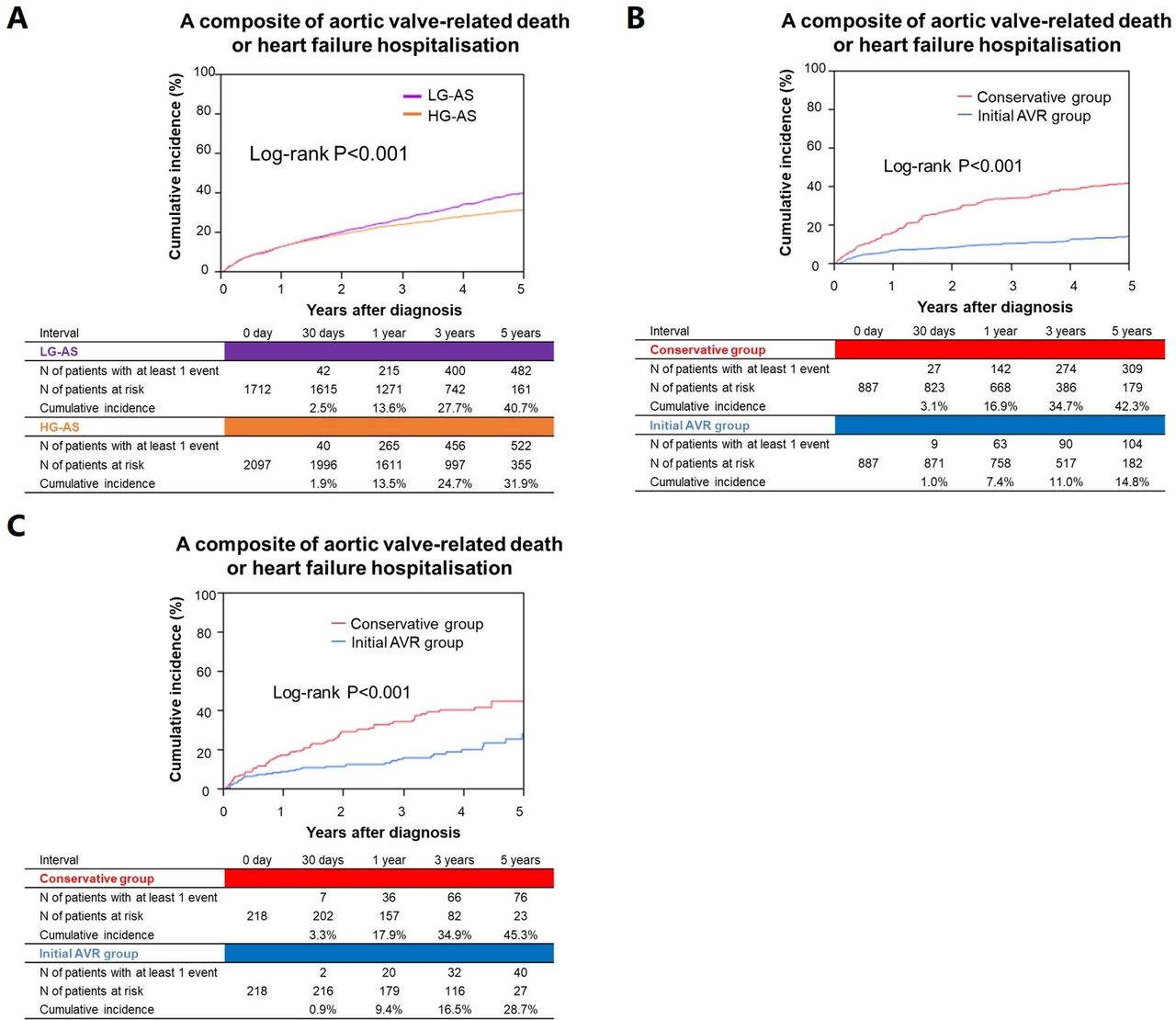
Some patients are classified as severe AS on the basis of AVA<1.0 cm2 alone with less severe Vmax and mean aortic PG. The clinical outcomes and management of patients with LG-AS, particularly with preserved LVEF, remain controversial. Patients with LG-AS are frequently encountered, but infrequently treated with AVR in the real clinical practice.52 In the CURRENT AS registry, patients with LG-AS were much older and more often had comorbidities such as diabetes, hypertension, previous stroke, renal failure, atrial fibrillation and coronary artery disease.53 Patients with LG-AS had higher rates of the composite of aortic valve-related death or HF hospitalisation as compared with those patients with high-gradient severe aortic stenosis (HG-AS) (figures 5 and 6).53 54 Initial AVR strategy was associated with better long-term clinical outcomes than conservative strategy in both patients with HG-AS and patients with LG-AS, although AVR was less frequently performed in patients with LG-AS than in patients with HG-AS (figure 5). We also showed the favourable effect of initial AVR strategy in patients with LG-AS with LVEF≥50%, although we could not distinguish patients with paradoxical low-flow LG-AS from those with normal-flow LG-AS because we did not collect data on the stroke volume. Therefore, the initial AVR might be a viable option in some patients with LG-AS and preserved LVEF, though the definitive conclusion could not be drawn because no randomised controlled trials have been done in these patients. Patients with LG-AS often have less severe AS than patients with HG-AS.12 One of the postulated mechanisms for the improvement of clinical outcomes with AVR in patients with LG-AS might be the effect of left ventricular unloading provided by AVR in patients with left ventricular systolic and/or diastolic dysfunction.2 Considering the poor prognosis of patients with LG-AS, we should make every effort to find out those patients with LG-AS who could benefit from AVR. In this context, we should pay more attention to the assessment of the morphology and degree of the aortic valve calcification by echocardiography and/or CT to find out those patients with LG-AS who have truly severe AS.3 Most importantly, the clinical characteristics, severity of AS and clinical outcomes may be highly heterogeneous in patients with LG-AS. Therefore, the decision regarding AVR in patients with LG-AS should be made on an individual patient basis. Further investigation should be warranted for defining the optimal treatment strategies of patients with paradoxical low-flow LG-AS. The main findings of the CURRENT AS registry are summarised in online supplementary table 1.
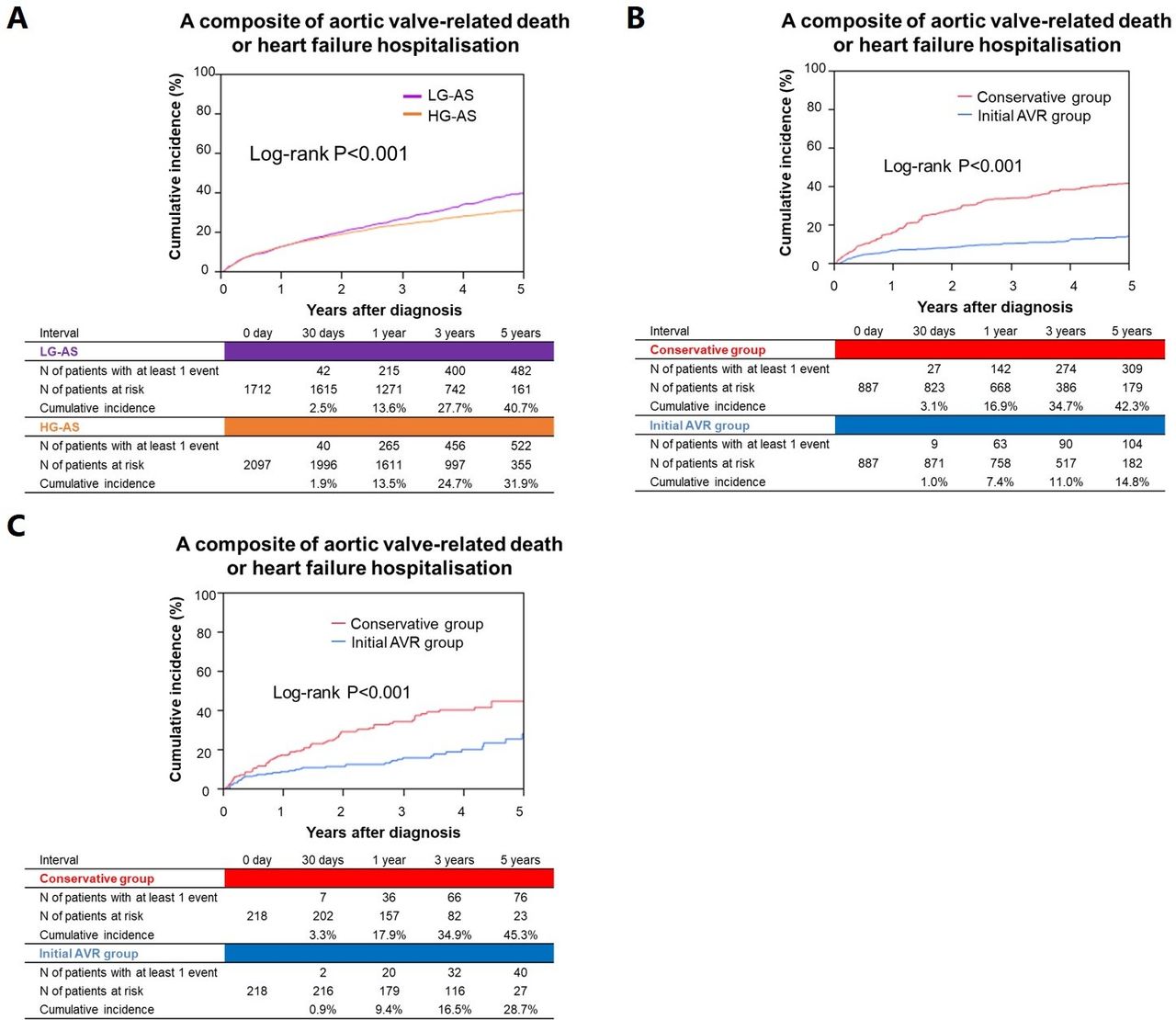
Cumulative incidences of a composite of aortic valve-related death or heart failure hospitalisation: (A) HG-AS versus LG-AS, (B) initial AVR versus conservative strategies in the propensity score-matched HG-AS stratum and (C) initial AVR versus conservative strategies in the propensity score-matched LG-AS stratum. Reprinted from Taniguchi et al 53 with permission from Wolters Kluwer Health. AVR, aortic valve replacement; HG-AS, high-gradient severe aortic stenosis, LG-AS, low-gradient severe aortic stenosis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distributions, rate of initial AVR, and clinical outcomes in HG-AS and LG-AS. AS, aortic stenosis; AVA, aortic valve area; AVR, aortic valve replacement; CURRENT AS, Contemporary Outcomes after Surgery and Medical Treatment in Patients with Severe Aortic Stenosis; HF, heart failure; HG-AS, high-gradient severe aortic stenosis, LG-AS, low-gradient severe aortic stenosis; LV, left ventricle; LVEF, left ventricle ejection fraction; PG, pressure gradient.
Conclusions
The observations from the CURRENT AS registry have provided important information on the demographics and clinical outcomes of patients with severe AS in real-world clinical practice just before introduction of TAVI in Japan. Prospective CURRENT AS Registry-2 is ongoing after introduction of TAVI in Japan (URL: http://www.umin.ac.jp/ctr/index.htm, unique identifier: UMIN 000034169).
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors have substantially contributed to the writing, research and design of this commissioned review. TT, TM and TK contributed substantially to the design, writing, concept and structure of the manuscript.
Funding This work was supported by an educational grant from the Research Institute for Production Development (Kyoto, Japan).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.